Background
Starr and Edwards described the first successful prosthetic valve replacement in 1961.
1 The ball-and-cage mechanical prosthesis was replaced by the (single) tilting disc valve in the 1970s and then, in the 1980s, by the St. Jude Medical bileaflet prosthesis. Although the durability of mechanical valves is superior, the risk of thromboembolic complications and bleeding related to anticoagulation has led to the widespread use of bioprosthetic valves, including porcine valves, homografts, and valves constructed from bovine pericardium.
Types of Prosthetic Valves
Just over half of implanted valves are mechanical, and of these, most are of the bileaflet tilting disc type.
Porcine aortic valve bioprostheses have been the most commonly implanted tissue valves, although bioprosthetic valves fabricated from xenograft pericardium, especially bovine, are becoming increasingly popular. Bioprosthetic valves are usually stented, but may lack a rigid structure and use, for example, porcine aorta as the valve ring.
Bioprosthetic valves are usually inserted during an open surgical procedure that may be minimally invasive or be inserted via a transcatheter approach, in the case of degenerative trileaflet aortic stenosis. Self- or balloon-expanding valves, in addition to transcatheter insertions, have been designed for surgical valve replacements, for ease of insertion with minimal if any suturing.
Tissue Valves
Tissue valves are either
xenografts or
homografts (
Table 178.1).
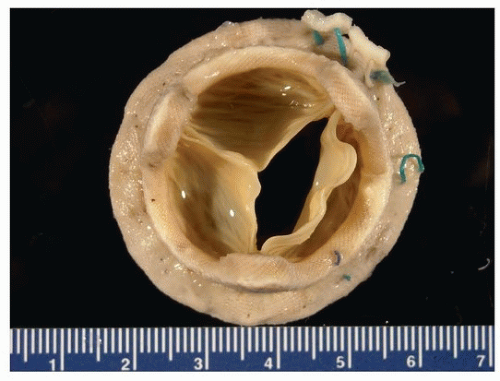
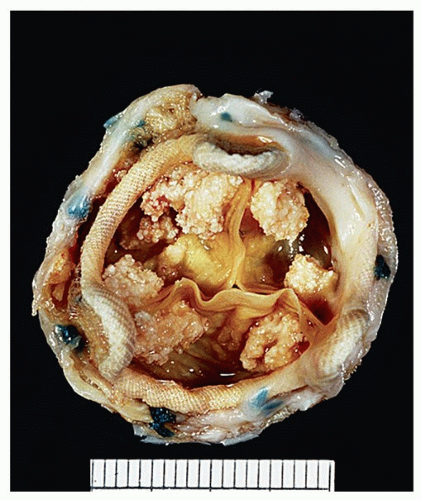
Xenografts are made from preserved animal tissues that are usually mounted on a fabric-covered prosthetic frame or stent (
Figs. 178.1,
178.2,
178.3). There are two common types, intact porcine aortic valves and valves constructed from bovine or porcine pericardium. The frame consists of posts (struts) and the intervening valve ring. Stentless xenografts are porcine aortic valves without a rigid stent and often have a portion of porcine aorta attached (full root valves) or lack porcine aorta (subcoronary valves).
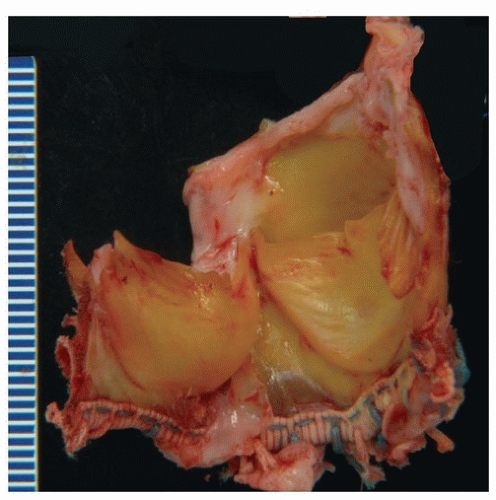
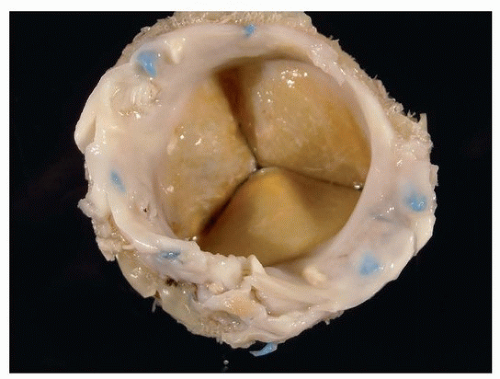
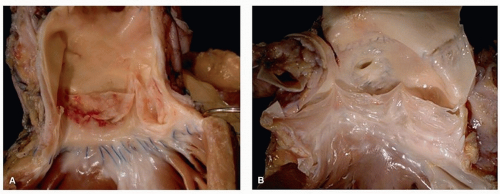
2Pericardial xenograft bioprostheses are made of bovine parietal pericardium that is produced by computer-aided design to simulate valve leaflets (
Figs. 178.4,
178.5,
178.6).
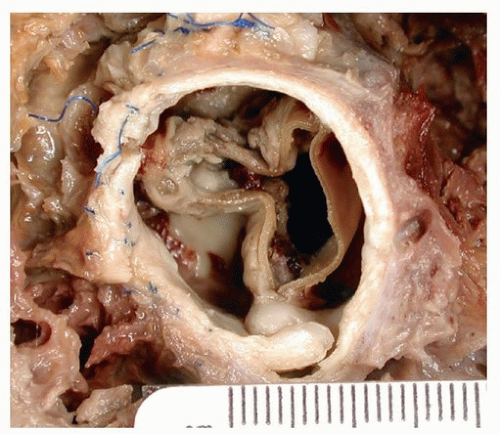
Homografts are human tissue grafts, generally cryopreserved allografts harvested from cadavers or from live donors. These are also stentless, or transplanted directly into the aortic root, without a supporting synthetic frame (
Fig. 178.7). Autografts are homografts derived from the patient, usually the pulmonic valve translocated to the aortic position in cases of congenital aortic stenosis.
A list of the more common bioprosthetic valves and their characteristics are presented in
Table 178.2.