Background
The aim of this study was to assess speckle tracking–derived fetal cardiac function in a normal population and in recipient fetuses of twin-to-twin transfusion syndrome (TTTS).
Methods
A case-control study was conducted of 59 uncomplicated singleton pregnancies and 17 recipient fetuses of TTTS. Peak systolic strain, strain rate, velocity, and displacement were calculated, corrected for gestational age, and compared between patients with TTTS and controls.
Results
The feasibility of speckle tracking was 83% in controls but only 61% in patients with TTTS. Myocardial velocity and displacement increased over gestation, and regional differences were present within each wall and between walls. Strain and strain rate were stable within each wall but were higher in the right ventricle than in the left ventricle and septum. Right ventricular strain was decreased in patients with TTTS compared with controls (0.75 ± 0.34 vs 1.00 ± 0.37 multiples of the median, P = .04).
Conclusion
The feasibility of speckle tracking is low when imaging conditions are challenging, but it can identify right ventricular failure in selected patients with TTTS.
Twin-to-twin transfusion syndrome (TTTS) complicates 9% to 15% of monochorionic diamniotic twin pregnancies. Different groups have shown that cardiac function in most recipient twins of TTTS is altered because of volume overload and/or endocrine dysregulation. Fetoscopic laser coagulation of the anastomosing placental vessels has been shown to cure TTTS and to improve recipients’ cardiac function. This finding has led many centers to perform thorough fetal cardiac functional assessment before and after laser therapy for research purposes, and some have even suggested introducing new clinical cardiac staging systems for TTTS.
Unfortunately, most of the methods used for the assessment of fetal cardiac function are flawed by high interobserver and intraobserver variability, involve extensive operator training, or require hardware that is not available on standard obstetric ultrasound machines (reviewed in Van Mieghem et al ).
Speckle tracking is a novel ultrasound tool to assess cardiac ventricular function. The method identifies myocardial “speckle patterns,” which are patterns in the acoustic backscatter generated by the reflected ultrasound beam on a 2-dimensional B-mode ultrasound image. The speckles are recognized in the subsequent frames of a cine-loop sequence and referenced back to their positions in the previous frame. On the basis of the data obtained, myocardial displacement can be “tracked,” and velocity vectors can be generated. Comparison of adjacent vectors then allows calculation of the actual displacement, velocity, deformation (strain), and velocity at which deformation occurs (strain rate) in the cardiac wall. The technique has been integrated in different software algorithms from different vendors and is now commercially available. The different algorithms have been validated against gold-standard methods to assess ventricular function both in animal models and humans, and their clinical relevance is at present being evaluated in the adult setting for different cardiac pathologies, such as hypertension, myocardial infarction, cardiomyopathy, diabetes, and (congestive) heart failure.
One of the major advantages of speckle tracking over (tissue) Doppler or M-mode cardiac function measurements is that the technology is relatively angle independent. Second, it requires the acquisition of only a short cine-loop sequence of the fetal cardiac 4-chamber view, which does not mandate any additional hardware, can be done by a sonographer with limited experience in fetal cardiology, and allows the exam to be “piggybacked” on any prenatal ultrasound exam. Finally, speckle tracking can be used to quantify fetal right ventricular function, which can only be partially achieved with other techniques because of the specific geometry and anatomy of this ventricle.
Early clinical experience in healthy fetuses, as well as in fetuses with congenital heart disease, showed a good feasibility and reproducibility of measurements. Therefore, speckle tracking could be a promising tool in the functional assessment of the fetal heart in TTTS. The aims of this study were to assess the feasibility and reproducibility of speckle tracking–derived cardiac function analysis in a population of healthy fetuses and to compare the findings with those in a cohort of recipient fetuses of TTTS.
Methods
Study Population
We performed this prospective case-control study at the University Hospitals Leuven (Leuven, Belgium) after approval of the protocol by the hospital ethics committee for clinical studies. All mothers gave informed consent for this study.
As a control group, we recruited 59 women with uncomplicated singleton pregnancies attending our routine prenatal clinic at a gestational age between 16 and 36 weeks. They received additional ultrasound examinations for the sole purpose of measuring fetal cardiac function. All fetuses were assessed only once. Maternal medical records, routine prenatal ultrasound examinations, delivery records, and pediatric discharge reports were reviewed to exclude pathologies that could have interfered with cardiac function (intrauterine growth restriction, gestational diabetes, congenital malformations, etc).
Patients were 17 consecutive recipient fetuses of TTTS assessed at our unit in the same time period. TTTS was defined as the presence of oligohydramnios in the donor twin with a deepest vertical amniotic fluid pocket ≤2 cm and polyhydramnios in the recipient fetus with a deepest amniotic fluid pocket ≥8 cm prior to 20 weeks and ≥10 cm after 20 weeks in a monochorionic diamniotic twin pregnancy. Patients were staged at presentation according to the Quintero classification system ( Figure 1 ), and fetal cardiac assessment was done before any therapeutic procedure was performed.

Cardiac Ultrasound
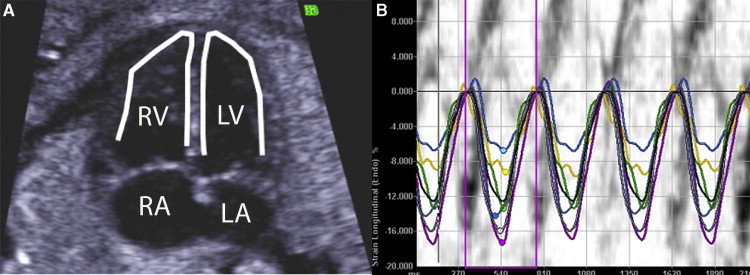
All ultrasound examinations were performed using a Voluson 730 Expert (GE Medical Systems, Kretztechnik, Zipf, Austria) ultrasound device using a 4-MHz to 8-MHz abdominal probe. On the basis of preliminary experiments (data not shown), machine settings were optimized for speckle tracking: speckle reduction imaging was turned off, and contrast and gain were optimized to show a clear delimitation of the ventricular wall. A fetal 4-chamber view was obtained, and the image was magnified as much as possible to include only the fetal heart. The latter is particularly important to achieve adequately high frame rates. Similar to what is done in postnatal echocardiography, we preferentially obtained a slightly angled apical or basal 4-chamber view so that the left ventricular free wall, the septum, and the right ventricular free wall were all clearly delineated ( Figure 2 A). A cine-loop sequence including 3 to 5 complete cardiac cycles was then recorded in the absence of fetal and maternal movements. Images were exported from the ultrasound machine in Digital Imaging and Communications in Medicine format and exported to a workstation running Syngo VVI (Siemens Medical Systems, Erlangen, Germany). Gating was performed on a concomitantly generated M-mode tracing of the mitral valve. The endocardium of the left and right cardiac ventricles was manually traced on a still frame in midsystole to end-systole. Tracing was started just below the atrioventricular valve annulus and then ran over the ventricular free wall, along the apex, and then back to the cardiac base over the septum ( Figure 2 A). Only the muscular part of the septum was included in the trace. The algorithm then automatically tracked the endocardium on the basis of speckle tracking and border recognition and displayed this in a cine-loop clip. The accuracy of tracking was subjectively verified and corrected when necessary. Velocity vectors were generated by the software, and peak longitudinal cardiac velocity, displacement, strain, and strain rate were calculated for 3 segments per ventricular wall (base, mid, and apex; Figure 2 B). Although we tracked both the left and right endocardial sides of the septum with this method, we arbitrarily chose to use only data obtained from the left side for this study, as both are reflections of the same muscular region ( Figure 2 A).
Interobserver variability was tested for longitudinal peak systolic strain and strain rate in the left ventricular free wall (averaged value of the 3 regions) in 15 randomly selected control subjects by 2 observers (T.V.M. and S.G.) unaware of each other’s measurements tracing the same data set. Intraobserver variability was tested by one observer (T.V.M.) tracing the same data set twice on different days.
Patients with TTTS additionally underwent fetal cardiac function evaluation by means of the right and left ventricular myocardial performance index, Doppler assessment of ductus venosus and umbilical vein flow, and assessment of atrioventricular valve regurgitation as previously described.
Statistical Analysis
Statistical analysis was performed using JMP version 7.0 (SAS Institute Inc, Cary, NC) and Prism for Windows version 5.0 (GraphPad Software, San Diego, CA). The normality of the data was assessed using the D’Agostino omnibus test. All variables were normally distributed. The presence of regional differences in the examined indices was evaluated using two-way analysis of variance and Bonferroni’s post hoc test for P < .05. Data were subsequently averaged per wall, and correlations between the variables and gestational age in the control group were evaluated using Pearson’s correlation coefficient and linear regression analysis. To adjust for gestational age, averaged variables were subsequently transformed to multiples of the median on the basis of the linear regression equation. Patients with TTTS were then compared with controls using two-sample Student’s t tests. All tests were two sided. A P value < .05 was considered statistically significant.
Interobserver and intraobserver variability were assessed using Bland-Altman analysis, plotting the difference between two observations expressed as a percentage of the mean of both observations on the y-axis versus the mean of both observations on the x-axis.
Results
Control Fetuses
Fifty-nine controls were recruited for the study. The mean gestational age at ultrasound was 24.4 weeks (range, 16.9-36 weeks). Adequate cardiac 4-chamber view cine-loop clips could be obtained in 55 fetuses (93%), with frame rates ranging from 60 to 110 Hz. The fetal heart could not be visualized adequately in 2 cases because of fetal position and in 2 because of maternal obesity. Fifty-five fetuses theoretically yield 495 cardiac segments to track (3 segments per cardiac wall, 3 walls per fetus). However, visually adequate tracking was obtained in only 440 segments (89%). Overall feasibility was therefore 81% (89% of 93%). Regional differences were present for velocity and displacement ( Table 1 , Figure 3 ). Both indices increased from the apex to the base. Moreover, these indices were significantly higher in the right ventricular free wall than in the septum and the left ventricular free wall (Bonferroni P < .0001 for both). Strain and strain rate did not show regional differences within each wall but were higher in the right ventricular free wall than in the septum (Bonferroni P < .05) and the left ventricular free wall (Bonferroni P < .01).
| Left ventricle | Septum | Right ventricle | 2-way analysis of variance P value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Base | Mid | Apex | Base | Mid | Apex | Base | Mid | Apex | Wall | Region |
| Velocity (cm/s) | 1.3 ± 0.6 | 0.9 ± 0.5 | 0.5 ± 0.3 | 1.3 ± 0.6 | 0.7 ± 0.5 | 0.3 ± 0.2 | 1.9 ± 0.7 | 1.4 ± 0.6 | 0.8 ± 0.5 | <.0001 | <.0001 |
| Displacement (mm) | 1.3 ± 0.6 | 0.9 ± 0.5 | 0.5 ± 0.4 | 1.3 ± 0.7 | 0.8 ± 0.5 | 0.4 ± 0.3 | 2.2 ± 0.9 | 1.6 ± 0.8 | 0.9 ± 0.6 | <.0001 | <.0001 |
| Strain (%) | −15.1 ± 7.5 | −13.9 ± 6.4 | −15.1 ± 7.7 | −14.7 ± 8.1 | −14.8 ± 5.9 | −17.7 ± 8.1 | −19.1 ± 8.4 | −18.0 ± 9.3 | −18.0 ± 10.1 | .0002 | .33 |
| Strain rate (s −1 ) | −1.8 ± 1.0 | −1.7 ± 0.7 | −1.8 ± 0.9 | −1.8 ± 1.1 | −1.8 ± 0.7 | −2.1 ± 1.1 | −2.4 ± 1.1 | −2.3 ± 1.1 | −2.2 ± 1.2 | <.0001 | .68 |

Peak systolic velocity and displacement were strongly correlated with gestational age in the 3 cardiac walls we assessed ( Table 2 , Figures 4 ; all P values < .05). Peak systolic strain and strain rate were independent of gestational age in the left ventricle ( R 2 = 0.02 and 0.05, P = .37 and .09, respectively) and the septum ( R 2 = 0.00001 and 0.01, P = .98 and .46, respectively). Strain rate decreased slightly with gestational age in the right ventricle ( R 2 = 0.13, P = .01). The regression formulas defining peak systolic velocity and displacement in all walls as well as right ventricular strain are presented in Table 2 .
| Correlation with GA | |||||
|---|---|---|---|---|---|
| Variable | P | R 2 | Regression formula | Mean | SD |
| Left ventricle | |||||
| Displacement | .002 | 0.17 | y = −0.010127 + 0.0394113 × GA | 0.94 | 0.49 |
| Velocity | .001 | 0.18 | y = 0.1456676 + 0.0328193 × GA | 0.94 | 0.40 |
| Strain | .37 | 0.02 | — | −15.1 | 5.2 |
| Strain rate | .09 | 0.05 | — | −1.82 | 0.68 |
| Septum | |||||
| Displacement | .0001 | 0.26 | y = −0.319136 + 0.0488245 × GA | 0.86 | 0.49 |
| Velocity | <.0001 | 0.32 | y = −0.29961 + 0.0447839 × GA | 0.79 | 0.41 |
| Strain | .98 | 0.00001 | — | −16.1 | 5.2 |
| Strain rate | .46 | 0.01 | — | −1.95 | 0.69 |
| Right ventricle | |||||
| Displacement | .02 | 0.12 | y = 0.4839138 + 0.0477055 × GA | 1.62 | 0.71 |
| Velocity | .01 | 0.13 | y = 0.4689877 + 0.0378291 × GA | 1.37 | 0.54 |
| Strain | .09 | 0.06 | — | −18.5 | 6.8 |
| Strain rate | .01 | 0.13 | y = −3.899211 + 0.0637494 × GA | −2.37 | 0.93 |




