♦ the incidence of cardiovascular disease in the United States
♦ modifiable and nonmodifiable risk factors for cardiovascular disease
♦ strategies for preventing cardiovascular disease.
Understanding cardiovascular disease
Cardiovascular disease (CVD) is a term used to describe various conditions that affect the structure and function of the heart and blood vessels. Common types of CVD include:
• coronary artery disease (CAD)
• heart failure
• cerebrovascular disease
• peripheral artery disease
• ischemic heart disease
• rheumatic heart disease
• congenital heart disease.
Heart-breaking numbers
• CVD is the leading cause of mortality and morbidity among men and women in the United States. Estimates indicate that more than 58 million people in the United States have CVD, costing the nation more than $108.9 billion on services, medications, and lost productivity.
• The Centers for Disease Control and Prevention (CDC) estimates that 600,000 people die each year in the United States due to coronary-related deaths.
• Nine hundred thirty-five thousand people experience a myocardial infarction every year (1 in 4 die).
Hocus focus
Prevention and risk reduction strategies for CVD tend to focus on atherosclerotic disease, or atherosclerosis. Atherosclerosis occurs when lipid deposits, thrombi, or calcifications cause inflammation and arterial wall changes.
Risk assessment
Atherosclerotic disease, which includes CAD, used to be considered a normal, inevitable part of the aging process. However, the Framingham Heart Study—which followed 5,209 healthy men and women for several years in search of characteristics shared by those who eventually developed CAD—identified factors to help assess a patient’s risk of CAD. Now, a Framingham Risk Score is an important part of caring for patients who have or are at risk for CAD. Knowing a patient’s risk can guide health care providers to plan interventions that may help prevent or reduce the patient’s risk of developing atherosclerotic disease.
What’s the score?
The Framingham Risk Score estimates a patient’s risk of developing CAD by assigning a score to these patient factors:
• age
• total cholesterol level
• high-density lipoprotein (HDL) level
• low-density lipoprotein (LDL) level
• blood pressure
• presence or absence of diabetes mellitus
• smoking status.
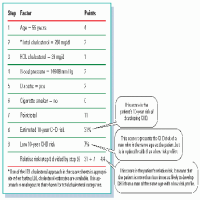
Individual risk factor scores differ for men and women and may be based on total cholesterol level or LDL cholesterol level. A patient’s total score (the sum of the individual risk factor scores) determines his 10-year risk of developing CAD. (See Table 3.1, Sample score sheet for estimating coronary heart disease risk.) The patient’s relative risk of developing disease can then be determined by comparing the patient’s score with the total scores of individuals of the same sex and age whose risk of CAD is average or low.
Table 3.1 is an example from the National Heart, Lung, and Blood Institute (NHLBI) that illustrates a sample score sheet for a 55-year-old man with a total cholesterol level of 250 mg/dl, a high-density lipoprotein cholesterol level of 39 mg/dl, and a blood pressure of 146/88 mm Hg. The patient also has diabetes and is a nonsmoker.
According to the NHLBI, practitioners should use the Total Cholesterol Score Sheet to determine coronary heart disease (CHD) risk when total cholesterol and HDL cholesterol levels are known; they should use the LDL Cholesterol Score Sheet when LDL cholesterol and HDL cholesterol levels are known.1
Source: National Heart, Lung, and Blood Institute, National Institute of Health. National Heart Lung and Blood Institute, National Institutes of Health. “Sample Score Sheet for Estimating Coronary Heart Disease Risk.” Available at http://www.nhlbi.nih.gov/about/framingham/risksamp.htm
Other applications
Researchers hope that ongoing research will provide evidence to support using the Framingham Risk Score for risk assessment of other atherosclerotic diseases, such as peripheral vascular arterial disease (associated with major limb loss) and cerebrovascular arterial disease.
Risk factors
Understanding the risk factors associated with CVD helps patients and health care providers develop strategies for prevention and risk reduction. Risk factors may be modifiable (controllable) or nonmodifiable (not controllable).
Nonmodifiable risk factors
Nonmodifiable risk factors for CVD include:
• advanced age
• sex
• heredity.
Advanced age
Although specific age-related changes may vary from person to person, individuals generally become more vulnerable to CVD with age. Complex organ systems start to decline, so other systems are forced to compensate.
With every beat of my heart
Age-related heart changes include:
• thickening and stiffening of the left ventricle
• fibrotic changes in the valves
• valve calcification
• increased reliance on atrial contractions to maintain cardiac output
• increased sensitivity to hypovolemia
• fibrotic changes in the bundle branches (a common cause of bundle-branch block in people older than age 65).
Vascular variations
Changes in the vascular system that tend to be age-related include:
• thickened intimal and medial layers of the arteries
• decreased arterial diameter
• stiffer, less elastic arterial walls due to calcium and lipid deposits.
These changes cause hypertension to develop.
Sex
Research has shown that men are at greater risk for developing CAD at a younger age than women. In men, risk increases beginning at age 45, whereas the risk in women increases after menopause (around age 55). Additionally, the lifetime risk of developing CAD is 1 in 2 for men and 1 in 3 for women.
Hormones: Helpful or hurtful?
Hormone replacement therapy for postmenopausal women was once thought to protect women from CVD. However, studies have shown that the risk of stroke, myocardial infarction (MI), and deep vein thrombosis increases with hormone replacement therapy.
Heredity
Researchers’ understanding of the complex relationship between genes and environmental factors in the development of CVD is in its infancy. However, many researchers believe that one-half of CVD cases can be attributed to genetic causes.
Genes on the scene
Genetics play a huge role in hypertension, heart disease, and other vascular conditions.
For example, some individuals with familial hypercholesterolemia (an inherited metabolic disorder affecting LDL receptors) carry a genetic mutation that makes it difficult for their cells to remove LDL from their blood. Patients with familial hypercholesterolemia have high serum cholesterol levels and are at risk for developing atherosclerosis.
History lesson
Obtaining a patient’s family history helps to identify patterns of early CVD and familial risk factors. For example, a patient has a higher risk of developing early CVD if he has a first-degree male relative who was diagnosed with CVD before age 55 or a female first-degree relative who was diagnosed with CVD before age 65. It is also likely that people with a family history of heart disease share common environments and risk factors that increase their risks.
Modifiable risk factors
Unfortunately, early development of CVD is commonly the result of lifestyle choices involving modifiable risk factors. Risk reduction strategies aim to reduce or eliminate the impact of these factors.
Smoking is the most common modifiable risk factor for CVD. In the United States, smoking causes almost as many deaths from heart disease as it does from lung cancer. The more a patient smokes and the longer he smokes, the higher his risk of CVD.
The damage done
Nicotine stimulates the sympathetic nervous system to constrict the arteries and raises blood pressure, which causes arterial wall damage. This damage promotes the formation of atherosclerotic plaque, causing tissues to become starved for oxygen. Exposure to secondhand smoke can increase the risk of heart disease for nonsmokers.
Only gold members can continue reading. Log In or Register to continue
 Just the facts
Just the facts