Compared with other preventive interventions, smoking cessation is extremely cost-effective. The more intensive the intervention, the lower the cost. Intensive counseling and the nicotine patch are particularly useful (Jama 1997;278:1759).
AHCPR recommendations: Every person who smokes should be offered smoking cessation treatment at every office visit. Cessation treatments even as brief as 3 min per visit are effective. More intense treatment is more effective in producing long-term abstinence. Three treatment elements, in particular, are effective, and one or more of these elements should be included in smoking cessation treatment: (1) nicotine replacement therapy (nicotine patches or gum), (2) social support (clinician-provided encouragement and assistance), and (3) skills training/problem solving (techniques on achieving and maintaining abstinence).
1 These factors are considered conditional risk factors when serum levels are abnormally high.
2 Obesity and physical inactivity are counted as major risk factors by the AHA. (Circ 2000;101:111)
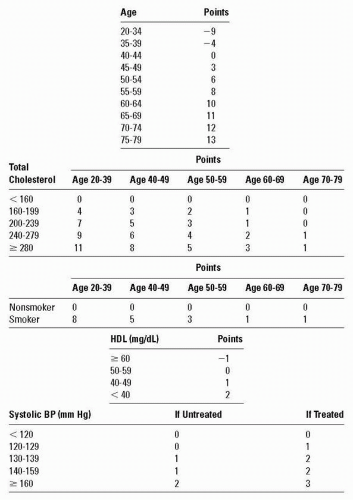
Figure 17.1 Calculation of CAD risk in men (ATP-III). (NIH)
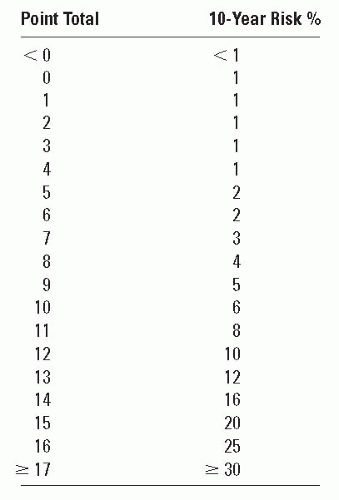
Figure 17.1 continued
Substantial evidence exists for risk factor clustering in smokers. Smokers are more likely than nonsmokers to have elevated lipids and HT (Circ 1997;96:3243).
Post-CABG, smokers 1 yr after surgery had more than twice the risk for MI and reoperation compared withpts who stopped smoking. Pts who were still smoking at 5 yr after surgery had even more elevated risks for MI, reoperation, and increased risk for angina. Pts who started to smoke again within 5 yr after surgery had increased risks for reoperation and angina. No differences in outcome were found betweenpts who stopped smoking since surgery and nonsmokers (Circ 1996;93:42).
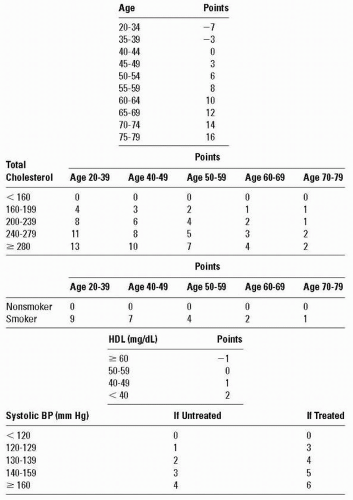
Figure 17.2 Calculation of CAD risk in women (ATP-III). (NIH)
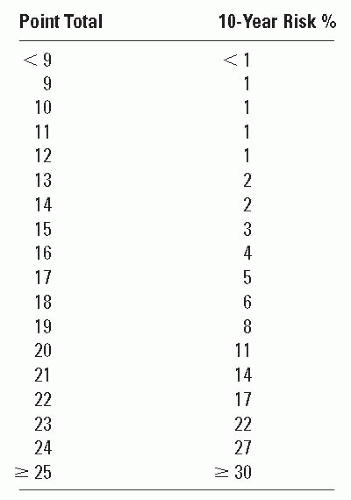
Figure 17.2 continued
Data on exposure to passive smoking as assessed by self-report suggest that regular exposure increases risk of CAD among nonsmoking women (Circ 1997;95:237).
Data on smokeless tobacco are inconclusive: Adverse CV effects are less than those caused by smoking but are greater than those found in non-tobacco users (Arch IM 2004;164:1845).
BP
HCTZ, atenolol, captopril, clonidine, diltiazem, and prazosin have no long-term adverse effects on plasma lipids. Previously reported short-term adverse effects from using HCTZ are limited to nonresponders (Arch IM 1999;159:551).
MRFIT (7-yr multifactor intervention program for lowering BP and serum cholesterol and for smoking cessation among high-risk men): At 16 yr, the intervention group had an 11.4% lower CAD mortality rate and a 20.4% lower rate for acute MI (Circ 1996; 94:946).
Lipids
The risk/benefit ratio supports use of statins in CAD. Elevated hepatic enzyme or CK levels < 10× nl require close monitoring but do not automatially mandate cessation of rx (Circ 2002;40:567).
In a study of 1017 young men followed 27-42 yr, the risk of developing CV disease in midlife correlated with earliest serum cholesterol levels (J Am Coll Cardiol 2002;40:2122; Nejm 1993;328:313). Statin therapy appears to be safe and effective in children with homozygous familial hyperlipidemia (Circ 2002;106:2231).
Inpts at high risk for development of CAD, LDL goal of < 70 mg/dL is a therapeutic option (J Am Coll Cardiol 2004;44:720).
In elderlypts (4736pts with mean age 72), baseline total, non-HDL, and LDL cholesterol levels and ratios of total, non-HDL, and LDL to HDL cholesterol are significantly related to CAD incidence. HDL cholesterol and triglycerides were not significant (SHEP program) (Circ 1996;94:2381).
In a small controlled study, cholesterol lowering with lovastatin produced a significant reduction in the number of episodes of ST-segment depression on AECG inpts with known ASHD (Circ 1997;95:324).
In middle-aged/elderly white men, a high level of fasting triglycerides is an independent risk factor for ASHD (Circ 1998;97:1029).
In a 5-yr prospective follow-up study of 2156 French Canadian men, Lp(a) was not an independent risk factor for ASHD but increased risk when associated with other lipid risk factors (J Am Coll Cardiol 1998;31:519).
Although current guidelines target reduction of LDL as the primary goal, rx ofpts with low HDL has been shown to reduce future event risk (Circ 2003;109:1809).
In all populations studied,pts who were prescribed lipid-lowering drugs remained without filled prescriptions for over 1/3 of the study year. After 5 yr, ˜50% of the surviving cohort had stopped using lipid-lowering rx altogether (Jama 1998;279:1458).
Activity
In a study of 25,714 adult men age 44 ± 10 yrs, low cardiorespiratory fitness was an independent predictor of CVD and all-cause mortality (Jama 1999;282:1547). In previously sedentary healthy adults, lifestyle and physical activity intervention was as effective as a structured exercise program in improving cardiorespiratory fitness and BP (Jama 1999;281:327). In the Physicians’ Health Study, habitual vigorous exercise reduced the risk of sudden death during exercise (Nejm 2000;343:1355).
In older (mean age 68 ± 5 yr)ptss/pMI, CABG, peak aerobic capacity improves with aerobic conditioning. The mechanism appears to be associated with peripheral skeletal muscle adaptations with no discernible improvements in CO (Circ 1996;94:323).
Regular weekly exercise can improve lipid profile independent of weight loss (Nejm 2002;347:1483). Walking and vigorous exercise are associated with a reduction in the incidence of CV events in postmenopausal women (Nejm 2002;347:716).
In a study of men with known ASHD who were enrolled in a program of physical exercise and low-fat diet, coronary stenoses progressed at a significantly slower rate than in the control group. Angiographic changes appeared to be largely due to chronic physical exercise (Circ 1997;96:2534).
Women with heart disease participating in a cardiac rehab program showed a 38% decrease in total cholesterol/HDL cholesterol over 5 yr (14% decrease in men). Total cholesterol decreased 20% in women and 8% in men, and LDL cholesterol decreased 34% in women and 15% in men (Circ 1995;92:773).
In a Finnish twin cohort study, leisure-time physical activity was associated with reduced mortality even after genetic and other familial factors were taken into account (Jama 1998;279:440).
Ornish: Intensive lifestyle changes may lead to regression of coronary atherosclerosis after 1 yr. More regression occurred after 5 yr than after 1 yr in an experimental group, while coronary atherosclerosis continued to progress and more than twice as many cardiac events occurred in controls (Jama 1998;280:2001).
Exercise Prescription
If an individual is < 40 yr old and asymptomatic, no further workup is needed. If an individual is > 40 yr old, an exercise test is recommended if vigorous exercise is planned. If test is normal, no further restrictions are needed. If test is abnormal, the individual should be treated as if he/she has CAD. If the pt has no known CVD but major risk factors or sx that suggest CAD, an exercise test is needed.
In the absence of ischemia/significant arrhythmias, exercise intensity should approximate 50-80% of VO2max, as ascertained by exercise test (use target of 20 beat/min above resting HR until test performed); target HR is 50-75% of heart rate reserve:
Target work intensity: Achieve training HR after 5-10 min of steady-state workload, expressed in METs. For walking on a level surface, activity can be prescribed as the step rate found on a treadmill to generate the desired HR.
Only gold members can continue reading. Log In or Register to continue