Good aerobic fitness is associated with favorable cardiovascular outcomes. However, it is not well known whether aerobic fitness correlates to the degree of coronary atherosclerosis, which affects cardiovascular prognosis. The aim of the present study was to investigate the relation between aerobic fitness and coronary atherosclerosis. A total of 8,565 apparently healthy men underwent routine health screening, including both cardiopulmonary function testing and coronary calcium scoring. The subjects with clinical cardiovascular disease or abnormal exercise electrocardiographic findings were excluded. A treadmill exercise test was done using the modified Bruce protocol, and the Agatston coronary artery calcium (CAC) score was measured using multidetector computed tomography. Advanced CAC was defined as a score >75th percentile according to the age group. The mean age was 51 ± 7 years, the average maximum oxygen uptake was 32 ± 5 ml/kg/min, and 34% had a positive CAC score. On univariate analysis, age, blood pressure, lipid profile, body mass index, hemoglobin A1c, fasting glucose, calculated 10-year risk for coronary disease, and maximum oxygen uptake were significantly associated with advanced CAC. In the multiple logistic regression model, the subjects in the highest quartile of the maximum oxygen uptake for age were less likely to have advanced CAC for age compared to those in the lowest quartile (odds ratio 0.60, 95% confidence interval 0.48 to 0.73), with adjustment for age, hypertension, hemoglobin A1c, current smoking, body mass index, and regular exercise habit. In conclusion, greater aerobic fitness was associated with less prevalent advanced coronary atherosclerosis in an asymptomatic male population. The degree of subclinical coronary artery disease might be 1 of the mechanisms connecting aerobic fitness and cardiovascular outcome.
Data on the association between exercise habits and/or aerobic fitness and coronary atherosclerosis in an asymptomatic population are scarce and inconsistent. Desai et al reported that advanced coronary artery calcium (CAC) is more prevalent in the sedentary group than those who are more physically active and adding physical inactivity to conventional risk factors improved the prediction of advanced CAC. The Coronary Artery Risk Development in Young Adults (CARDIA) study reported a significant association between coronary artery calcification and aerobic fitness in young adults. In contrast, data from the Heinz Nixdorf Recall study showed that exercise capacity correlated inversely with the CAC score on univariate analysis, but it was not significant after adjustment for age, gender, and other risk factors. Wilund et al reported no association between physical activity and coronary artery calcification in a small-scale study. We investigated the relation between aerobic fitness and coronary atherosclerosis in an asymptomatic population evaluated by maximal oxygen uptake (VO 2 max) during a treadmill exercise test and CAC score using multidetector computed tomography.
Methods
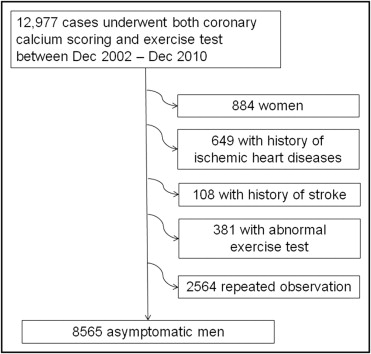
The study subjects were retrospectively chosen from those who participated in a health screening program at the Center for Health Promotion in Samsung Medical Center (Seoul, Republic of Korea) and underwent both exercise testing and coronary calcium scoring from December 2002 to December 2010. Because the number of female subjects was small among this group, we included only the male subjects to reduce confounding. Patients with a history of stroke or ischemic heart diseases or those with abnormal findings from the exercise test were excluded. Finally, the exclusion of repeated observations resulted in a final study population of 8,565 men ( Figure 1 ) . The institutional review board at the Samsung Medical Center (Seoul, Republic of Korea) approved the present study.
The body weight and height, blood pressure, and blood chemistry were obtained. Hypertension was defined as a systolic blood pressure >140 mm Hg or diastolic blood pressure >90 mm Hg or a history of being diagnosed with hypertension or taking antihypertensive medications. Diabetes was defined as a fasting blood glucose level of >7.0 mmol/L or hemoglobin A1c >6.5% or a history of being diagnosed with diabetes or taking medication for diabetes. A questionnaire was completed to obtain lifestyle factors such as smoking, alcohol intake, and habitual physical activity. The 10-year absolute risk of coronary events was calculated using the Framingham risk score.
All subjects were examined using the multidetector computed tomography system, Brilliance 40 (Phillips Medical Systems, Cleveland, Ohio) or VCT LightSpeed 64 (GE Healthcare, Milwaukee, Wisconsin). An analysis of the scans was performed on the workstation, Extended Brilliance Workspace (Phillips Medical System), or Advantage Windows (GE Healthcare). The Agatston score was used to estimate the degree of coronary calcification. The subjects were divided into 5 risk categories using the Agatston score: 0, 0 to 9, 10 to 99, 100 to 399, and ≥400. The subjects were grouped by age into 5 groups: <50, 50 to 54, 55 to 59, 60 to 64, and ≥65 years. A CAC score >75 percentile for each age group was defined as “advanced CAC” for subject age.
The treadmill exercise test (Quinton Q4500, Cardiac Science, Bothel, WA) was done by modified Bruce protocol. The blood pressure was measured manually using a mercury sphygmomanometer before and at the end of each stage of exercise. Electrocardiogram, heart rate, and oxygen consumption were also obtained. A tightly sealed breath mask connected to an airflow sensor was used. The respiratory gas analysis was done using dynamic breath-by-breath measurement using the Jaeger system (VIASYS Healthcare, Hoecherg, Germany). Various respiratory parameters, including minute ventilation, oxygen uptake, and carbon dioxide output, were measured with a sampling interval of 8 seconds to determine the VO 2 max. The subjects with positive finding (significant ST changes, blood pressure decrease, or arrhythmia during the test) were excluded from the study. Otherwise, the test was stopped according to the usual criteria for exercise testing: (1) exhaustion, (2) reaching >90% of the maximum heart rate (220 − age), (3) respiratory quotient ≥1.15, and (4) plateau of oxygen consumption. During the test, the subjects were allowed to lay their hands on the front bar lightly but not to grip strongly or lean on the front bar. The subjects were grouped by age into 5 groups (<50, 50 to 54, 55 to 59, 60 to 64, and ≥65 years), and the quartiles of VO 2 max were obtained for each age group.
Descriptions of the variables that showed a standard distribution were noted by the mean ± standard deviation, and the others by median representation. Because the CAC score had an extremely skewed distribution with a highly prevalent 0 score, and even a log transformation resulted in a distribution still significantly deviated from normal, Spearman’s correlation was used to evaluate the association between CAC and the other continuous variables. Otherwise, CAC was analyzed as a binary categorical variable (advanced CAC vs no advanced CAC). The chi-square test was used to test the association between advanced CAC and other variables, and a trend analysis was performed using the Cochran-Armitage trend test. Exploration of multiple logistic regression models was done to identify the independent predictors of advanced CAC. The initial model included age and VO 2 max as independent variables. The sequential addition of hypertension, diabetes mellitus, smoking status, hemoglobin A1c, lipid profile, C-reactive protein, body mass index, and exercise habits was done. The variables that contributed to an increase in the explanatory power of the model were retained. p Values <0.05 were considered statistically significant. All statistical analyses were performed using Stata/MP, version 11.2, for Windows (StataCorp, College Station, Texas).
Results
The clinical characteristics of the study subjects are listed in Table 1 . They were middle-age men, and the ethnicity was 100% Korean. The CAC score showed an extremely skewed distribution with a median of 0 and range of 0 to 3,324. The proportion of current smoking, hypertension, and diabetes was greater in the group with advanced CAC than in the group without it. Those with an exercise habit of ≥3 times/week were more likely to have advanced CAC than those with a lower exercise frequency.
| Variable | All Patients | Advanced CAC | p Value | |
|---|---|---|---|---|
| Yes (1,917) | No (6,648) | |||
| Age (years) | 51 ± 7 | 53 ± 6 | 50 ± 7 | <0.001 |
| Men | 100% | |||
| Smoking | <0.001 | |||
| Never | 23% | 19% | 24% | |
| Past | 45% | 45% | 45% | |
| Current | 32% | 36% | 31% | |
| Hypertension | 48% | 60% | 45% | <0.001 |
| Diabetes mellitus | 27% | 33% | 26% | <0.001 |
| Coronary calcium score | ||||
| 0 | 66% | |||
| 1–9 | 12% | |||
| 10–99 | 15% | |||
| 100–399 | 5% | |||
| ≥400 | 2% | |||
| Exercise frequency ≥3/week | 49% | 54% | 48% | 0.001 |
| Alcohol intake ≥3/week | 25% | 26% | 24% | NS |
| Maximal oxygen consumption (ml/kg/min) | 32 ± 5 | 31 ± 5 | 33 ± 5 | <0.001 |
| Duration of exercise (s) | 582 ± 88 | 586 ± 118 | 581 ± 79 | 0.06 |
| Body mass index (kg/m 2 ) | 24.8 ± 2.6 | 25.3 ± 2.7 | 27.7 ± 2.6 | <0.001 |
| Low-density lipoprotein cholesterol | NS | |||
| mg/dl | 126 ± 30 | 127 ± 31 | 126 ± 29 | |
| mmol/L | 3.3 ± 0.8 | 1.7 ± 1.0 | 1.7 ± 1.0 | |
| High-density lipoprotein cholesterol | <0.001 | |||
| mg/dl | 50 ± 12 | 50 ± 12 | 51 ± 12 | |
| mmol/L | 1.30 ± 0.32 | 1.28 ± 0.32 | 1.31 ± 0.32 | |
| Triglycerides | <0.001 | |||
| mg/dl | 150 ± 87 | 159 ± 90 | 148 ± 86 | |
| mmol/L | 1.7 ± 1.0 | 1.8 ± 1.0 | 1.7 ± 1.0 | |
| Fasting glucose | <0.001 | |||
| mg/dl | 99 ± 21 | 104 ± 26 | 97 ± 19 | |
| mmol/L | 5.5 ± 1.2 | 5.7 ± 1.4 | 5.4 ± 1.1 | |
| Hemoglobin A1c (%) | 5.6 ± 0.8 | 5.8 ± 1.0 | 5.6 ± 0.7 | <0.001 |
| Systolic blood pressure (mm Hg) | 119 ± 16 | 122 ± 16 | 119 ± 15 | <0.001 |
| Diastolic blood pressure (mm Hg) | 76 ± 11 | 78 ± 10 | 76 ± 11 | <0.001 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


