In preparation for catheter-based ablation of atrial fibrillation (AF), a significant amount of pertinent information should be collected to perform this procedure as safely as possible and avoid complications. Two facts should be always kept in mind: (a) atrial fibrillation is most commonly a relatively benign disease with the primary indication for ablation at this time being amelioration of symptoms and the reversal of tachycardia-induced cardiomyopathy in selected patients (1), and (b) catheter ablation is almost always an elective procedure. As such, AF ablation should be performed in ideal settings and under optimal conditions. In this chapter, we discuss all the pertinent data that should be considered and obtained prior to catheter ablation for AF.
Due to the potential risks of AF ablation, we typically evaluate all patients in the outpatient setting in order to discuss alternative approaches and therapies. At this time, all relevant details of the medical history should be explored, from type and duration of AF (paroxysmal, persistent, or permanent) to prior ablation(s), prior surgeries, medical conditions, medications, and allergies (1). Some of these factors can increase the morbidity of the procedure or increase the likelihood of AF recurrence after ablation (Table 4.1). For example, the presence of rods in the spine from scoliosis surgery can make visualization of the left atrium (LA) extremely difficult. In addition, a complete evaluation should be performed similar to any patient with new onset AF, including evaluation for reversible causes of AF (Table 4.2). Recent laboratory data should be reviewed to exclude abnormalities that could complicate the procedure or recovery, such as significant anemia, thrombocytopenia or coagulopathy, infection, renal insufficiency, and electrolyte disturbance.
A resting 12-lead electrocardiogram (ECG), a rhythm strip, and a 24-hour Holter or 30-day event monitor should be obtained to document atrial fibrillation. A cardiac ultrasound, at a minimum transthoracic or often transesophageal, should be obtained to document cardiac anatomy and function, such as LA size, left ventricular (LV) function and dimensions, valvular function, interatrial septal anatomy, and exclusion of possible anomalies or thrombus. Other imaging studies can also provide further detailed information about cardiac anatomy and function, such as cardiac computed tomography (CT) or magnetic resonance imaging (MRI) (see below). However, these studies are considered optional and may be used in selected patients dictated by clinical evaluation, institutional protocol, financial resources, procedural complexity, and specific ablation approach.
TABLE 4.1 Factors Most Likely Associated with Increased Morbidity of AF Ablation and Recurrence of AF
Anticoagulation (contraindications, adverse events, or complications)
Allergies (including IV contrast adverse effects)
Sedation history (complications and medical conditions)
TABLE 4.2 Reversible Causes of Atrial Fibrillation
Endocrinopathies
Thyroid disease
Carcinoid tumor
Pheochromocytomas
Infection/sepsis/fever
Cardiac
Pericarditis/myocarditis
Trauma
Obesity
Surgery (e.g., coronary bypass, valvular replacement, etc.)
Electrolyte disturbance
Pulmonary diseases
Sleep apnea
Hypoxia
Pulmonary embolism
Drugs
Cocaine
Amphetamines
Ethanol intoxication
A thorough evaluation of patients includes a discussion of alternative therapies, including rate control and anticoagulation strategy, a pace and ablate strategy, and surgical procedures.
ECG and Ambulatory ECG Recordings
A resting 12-lead ECG and rhythm strip should be performed to document AF. In the absence of AF, a 12-lead ECG will provide important information such as baseline sinus rate, QT interval, and possible triggers of AF, as well as exclude ongoing or active ischemia that would defer or postpone AF ablation.
The baseline sinus rate and QT interval are important to better select appropriate antiarrhythmic therapy if required during and/or immediately after the ablation. For example, propafenone, sotalol, and beta-blockers should be used cautiously in patients with significant bradycardia or tachy-bradycardia syndrome due to their significant negative chronotropic effect. Sotalol, dofetilide, ibutilide (class III antiarrhythmics) will significantly prolong QT interval, which can result in polymorphic ventricular tachycardia in susceptible patients.
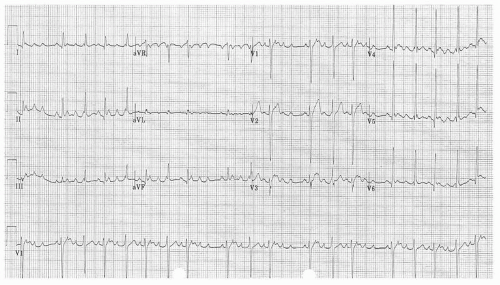
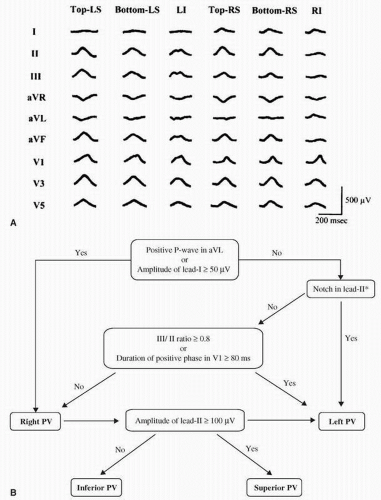
Triggers of AF have been well described. Tachycardia-induced tachycardia was described several decades ago, and refers to one tachycardia that can degenerate or transform into a second tachycardia. Examples of tachycardias that may precipitate AF include atrial tachycardia, atrioventricular (AV) nodal reentrant tachycardia (AVNRT), AV reentrant tachycardia (AV accessory pathway), and premature atrial contractions (2). These triggers may be potentially recognizable with a 12-lead ECG (Fig. 4.1) or ambulatory ECG recordings (24-hour Holter or 30-day event monitor; Fig. 4.2). Atrial ectopy that triggers AF has been documented to originate from the pulmonary veins (PVs), left atria (LA), vein of Marshall, crista terminalis, superior vena cava (SVC), and coronary sinus (CS) (3, 4, 5). The frequency of triggers and the site of triggers may be higher in younger patients. For example, a study in adolescents with documented AF and structurally normal hearts was found to have more underlying supraventricular arrhythmias (4). The P-wave axis and morphology in a 12-lead ECG can more precisely identify the source of atrial ectopy and focal tachycardia. Several studies have described the ECG P-wave morphology that accurately localizes the source of atrial ectopy and/or tachycardia (Fig. 4.3) (6, 7, 8, 9). Haissaguerre et al. described an algorithm based on P-wave morphology to identify the PV origin of atrial ectopic beats with an accuracy of 79% (Fig. 4.4) (9).
Figure 4.1. Right superior pulmonary vein tachycardia recorded from an 18-year-old male with AF.
Figure 4.2. Holter and 30-day event monitor in two different patients (A, B) with atrial ectopy/atrial tachycardia that degenerates to AF.
An attempt to control and treat such triggers should be made in order to better avoid recurrences of AF and to allow the electrophysiologists to focus on an area that may require further attention (10). In some centers, eliciting triggers during electrophysiologic study in patients referred for AF ablation is a critical component of the procedure. Sauer et al. demonstrated that slow-pathway ablation alone (without PV isolation) in patients referred for AF ablation with inducible AVNRT during electrophysiologic study had a very low rate of AF recurrence without antiarrhythmic drugs after 21 months (2). Other groups have reported similar results in small numbers of patients. Similarly, Haissaguerre et al. and multiple other groups have shown that successful catheter ablation of accessory pathways prevents further recurrence of AF in 91% of patients (11).
In patients with intermittent symptoms, a Holter or event monitor, as well as 12-lead ECG during symptoms, accurately diagnose AF and avoid misdiagnosis of other arrhythmias, which would require a different procedure or therapy. Dixit et al. demonstrated that AF could be erroneously diagnosed in patients with dual AV nodal pathways manifesting with double response and/or AVNRT (12). In another study, almost 10% of ECGs interpreted as showing AF were incorrectly classified (13). In addition, ambulatory ECG recordings will correlate symptoms with paroxysms and burden of AF. Ambulatory ECG recordings in patients with chronic AF are useful to assess ventricular rate and response to medical therapy, as well as to correlate symptoms associated with rapid ventricular response.
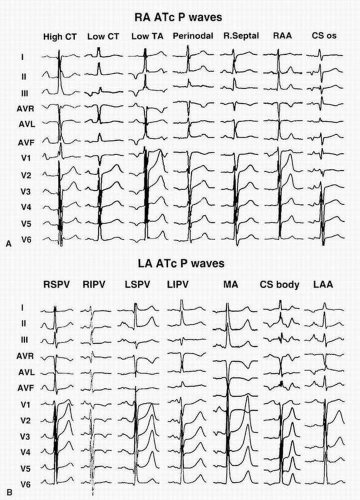
Figure 4.3. Representative examples of tachycardia P-wave morphology of tachycardias from right atrial sites (A) and left atrial sites (B). CT, crista terminalis; TA, tricuspid annulus; RAA, right atrial appendage; CS, coronary sinus; PV, pulmonary vein; RS, right superior; RI, right inferior; LS, left superior; LI, left inferior; MA, mitral annulus; LAA, left atrial appendage. (Reproduced with permission from Kistler PM, Roberts-Thompson KC, Haqqani HM, et al. P-wave morphology in focal atrial tachycardia: development of an algorithm to predict the anatomic site of origin. J Am Coll Cardiol. 2006;48:1010-1017.)
Figure 4.4. A: Surface ECG P-wave morphology in one patient with AF during pacing at six sites in four pulmonary veins. B: Algorithm to determine PV origin. For abbreviations refer to Figure 4.3. (Reprinted from Yamane T, Shah D, Peng JT, et al. Morphological characteristics of P waves during selective pulmonary vein pacing. J Am Coll Cardiol. 2001;38:1505-1510.)
Lastly, it is important to identify other co-existing conditions such as typical or atypical atrial flutter and other supraventricular arrhythmias, which would necessitate additional ablation and therefore will increase the complexity and time of the procedure.
Transthoracic and Transesophageal Echocardiogram
Transthoracic echocardiography (TTE) is paramount in the preprocedure evaluation of AF ablation. Detailed data on the cardiac function, anatomy, and possible anomalies will maximize the safety of the procedure, as well as provide information that can predict the response or failure of AF ablation.
The most important data pertinent to AF ablation include: (a) LA size; (b) LV dimension, thickness, and ejection fraction; (c) valvular function; (d) pulmonary artery pressure; (e) interatrial septum anatomy; (f) pericardial space and effusion; and (g) cardiac anomalies, if any exist.
The LA size can predict the response to AF ablation or direct the operator to perform more extensive LA substrate ablation. Studies have documented a higher AF recurrence rate after ablation in patients with larger LA size prior to the procedure. Hypertrophic cardiomyopathy may also have a higher AF recurrence rate after catheter-based ablation (14). Severe LV dilatation and depressed systolic function could facilitate volume overload and precipitate congestive heart failure during the ablation, particularly if an open-irrigated catheter is used. Additionally, knowledge of LV systolic function will guide appropriate antiarrhythmic drug selection in the pre-and postablation phase.
Special attention should be made to evaluate the right atrium and ventricle (e.g., abnormal insertion of the tricuspid valve may suggest Ebstein anomaly, which is associated with the presence of accessory pathways and trigger of AF). Moreover, pulmonary hypertension, congenital heart disease with significant shunts, and severe valvular heart disease are associated with a higher incidence of AF, and likely associated with a higher recurrence rate of AF after catheter ablation (no data available). The TTE will also provide a baseline evaluation of the pericardial space prior to ablation, to accurately diagnose any suspected acute complications during the ablation procedure, such as pericardial effusion and cardiac tamponade.
Only gold members can continue reading. Log In or Register to continue