Chapter 76 Pregnancy
Pulmonary Physiology
Physiologic Changes in Pregnancy
Hormonal changes in pregnancy affect the upper respiratory tract and cause airway hyperemia and edema resulting in symptoms of rhinitis. Estrogens are likely responsible for many of these effects because they produce capillary congestion and mucous gland hyperplasia. Changes to the thoracic cage result from both the enlarging uterus and the hormonal effects producing ligamentous laxity. The diaphragm is displaced cephalad by up to 4 cm, but the potential loss of lung capacity is partially offset by an increase in the anteroposterior and transverse diameters and by widening of the subcostal angle (Figure 76-1). Despite these anatomic changes, diaphragmatic function remains normal, diaphragmatic excursion is not reduced, and the maximum transdiaphragmatic inspiratory pressures that can be generated near term are similar to values generated by patients who are not pregnant. The changes in the chest wall return to normal within 6 months of delivery, although the costal angle may remain widened.
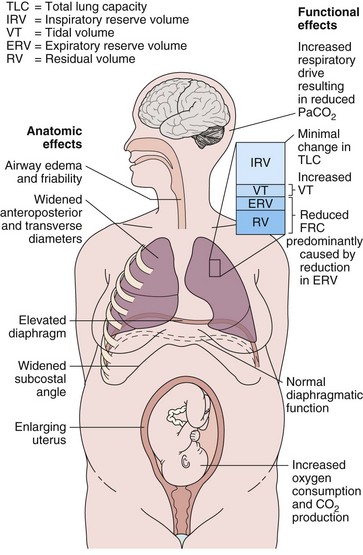
These changes in the thorax produce a progressive decrease in functional residual capacity (FRC) by 10% to 25% by term (Figure 76-2). Residual volume decreases slightly, but the major change is in expiratory reserve volume. These alterations are measurable as early as 16 to 24 weeks of gestation and progress to term. The increased diameter of the thoracic cage and the preserved respiratory muscle function allow the vital capacity to remain unchanged, and total lung capacity decreases only minimally. Measurements of airflow and lung compliance are not affected, but chest wall and total respiratory compliance are reduced in the third trimester because of the chest wall changes and increased abdominal pressure. Inconsistencies in results reported for diffusing capacity during pregnancy likely arise from the effects of anemia, variable changes in intravascular volume, and the increase in cardiac output. A small increase may be noted in early pregnancy with a subsequent decrease to normal values by term.
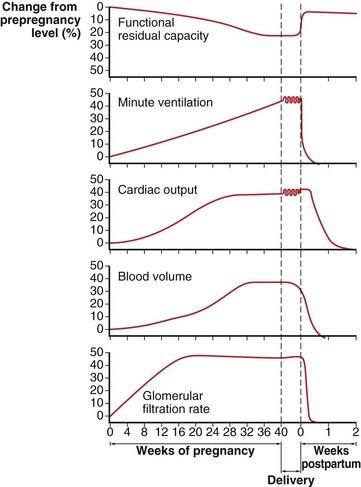
Minute ventilation increases greatly in pregnancy, beginning in the first trimester and reaching 20% to 40% above baseline at term (Figure 76-2), produced mainly by an increase in tidal volume of approximately 30% to 35%. These changes are mediated by the increase in respiratory drive that results from elevated serum progesterone levels. A respiratory alkalosis with compensatory renal excretion of bicarbonate results, with arterial carbon dioxide tension (PaCO2) falling to 28 to 32 mm Hg and plasma bicarbonate falling to 18 to 21 mEq/L. Alveolar-arterial oxygen tension difference (PO2[A−a]) is similar to nonpregnant values, and mean PaO2 usually exceeds 100 mm Hg at sea level throughout pregnancy. Mild hypoxemia and an increased PO2(A−a) may develop in the supine position because of airway closure, because FRC diminishes near term. One study suggests that shunt is normally increased in the third trimester to approximately 15% and is not changed significantly by posture. Oxygen consumption increases, beginning in the first trimester, and reaches 20% to 33% above baseline by the third trimester because of fetal demands and maternal metabolic processes. The combination of a reduced FRC and increased oxygen consumption lowers oxygen reserve, which renders the pregnant patient susceptible to the rapid development of hypoxia in response to hypoventilation or apnea.
Complications and Disorders of Pregnancy
Pregnancy-Specific Disorders
Amniotic Fluid Embolism
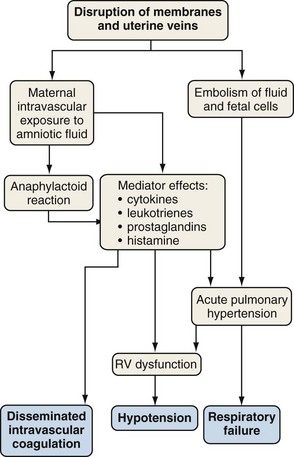
Amniotic fluid embolism is a rare obstetric complication (between 1 in 8000 and 1 in 80,000 live births) that carries a mortality rate of 10% to 86% and may account for 10% of maternal deaths. Amniotic fluid embolism is usually associated with labor and delivery, but it may also occur with uterine manipulations or uterine trauma or in the early postpartum period. The mechanism seems to involve amniotic fluid that enters the vascular circulation through endocervical veins or uterine tears. Particulate cellular contents and humoral factors in the amniotic fluid produce acute pulmonary hypertension, predominantly by causing vascular spasm (Figure 76-3). Acute right ventricular dysfunction results from the increased afterload and myocardial dysfunction mediated by humoral factors, associated with secondary left ventricular (LV) failure. The cardiovascular changes of amniotic fluid embolism may resemble those of anaphylaxis, and sensitivity to amniotic fluid contents may be responsible.
Preeclampsia and Pulmonary Edema
Pulmonary edema may rarely occur in association with preeclampsia (i.e., perhaps 3% of preeclamptic patients). The preeclamptic patient is usually volume-depleted, and pulmonary edema usually occurs in the early postpartum period, often associated with aggressive, intrapartum fluid replacement. Other factors that may contribute to the pathogenesis include reduced serum albumin, elevated LV afterload, and systolic and diastolic myocardial dysfunction (Figure 76-4). Increased capillary permeability may also occur, aggravated by concomitant conditions such as sepsis, placental abruption, or massive hemorrhage.
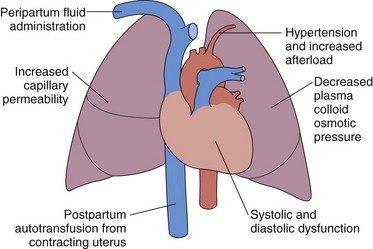
Figure 76-4 Pathophysiologic mechanisms responsible for the development of pulmonary edema in preeclampsia.
Tocolytic Pulmonary Edema
The clinical presentation is of acute respiratory distress with features of pulmonary edema. No specific features characterize tocolytic pulmonary edema. The diagnosis is a clinical one, made in the presence of acute pulmonary edema occurring in the appropriate clinical situation. The differential diagnosis includes cardiogenic pulmonary edema, amniotic fluid embolism, and other conditions (Table 76-1). Failure of the pulmonary edema to resolve in 12 to 24 hours requires a search for alternative causes.
Table 76-1 Acute Respiratory Distress Caused by Complications of Pregnancy and Labor
| Disorder | Distinguishing Features |
|---|---|
| Amniotic fluid embolism | Cardiorespiratory collapse, seizures, disseminated intravascular coagulation |
| Pulmonary edema caused by preeclampsia | Hypertension, proteinuria |
| Tocolytic pulmonary edema | Tocolytic administration, rapid improvement with discontinuation |
| Aspiration pneumonitis | Vomiting, aspiration |



