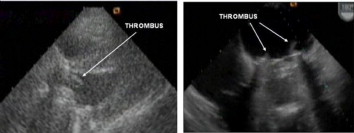
Pregnancy is associated with an increased risk of valve thrombosis in patients with metallic prosthetic heart valve (MHV). Warfarin treatment is the best regimen against thromboembolic complications, but its use in the first trimester can result in embryopathy. Low molecular weight heparin (LMWH) does not cause embryopathy. However, the pharmacokinetics of LMWHs change during pregnancy and serial monitoring of anti-Xa levels is strongly recommended. We present three cases of MHV thrombosis occurring while on therapy with LMWH during pregnancy. Case 1 was an 18-year-old female who had undergone mitral valve replacement (MVR) with a bileaflet MHV (Sorin 33 mm) and aortic valve replacement (AVR) with a bileaflet MHV (Sorin 23 mm). She was referred to our hospital in the 9th week of pregnancy with palpitation and acute neurological deficit in the left arm. She had been treated with subcutaneous enoxaparin, 70 mg twice daily, since the beginning of the pregnancy. Transthoracic and transesophageal echocardiography (TTE and TEE) depicted 6 mm fibrillar thrombus in the aortic prosthetic valve and thrombi in the mitral prosthetic valve (Figure). Case 2 was a 36-year-old female who had undergone MVR with a bileaflet MHV (Sorin 29 mm). She was admitted to our coronary care unit with pulmonary edema in the 33rd week of pregnancy. Subcutaneous enoxaparin had been initiated 60 mg twice daily since the beginning of her pregnancy. Urgent TTE and TEE demonstrated thrombi and a 10.5 mmHg mean gradient in the mitral prosthetic valve. Case 3 was a 25-year-old female who had undergone surgery MVR with a bileaflet MHV (Sorin 27 mm). She had been treated with subcutaneous enoxaparin, 60 mg twice daily, since the 2nd week of her pregnancy. She was admitted with New York Heart Association (NYHA) class II dyspnea for 10 days in the 21st week of pregnancy. TTE demonstrated thrombus and a mean gradient of 12 mmHg in the mitral prosthetic valve. The patient became symptomatic (NYHA class III dyspnea and palpitation) in the 34th week. Cesarean section was carried out. She had dyspnea at rest, palpitation and fatigue after the delivery. No change in the thrombus or the mean gradient (12 mmHg) was detected in the follow-up echocardiography. The patient underwent MVR after delivery. In conclusion, in the absence of anti-Xa monitoring, pregnants with MHV should not be treated with a fixed dose of LMWH, as such treatment likely results in ineffective anticoagulation.