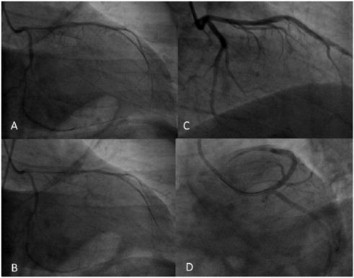
Coronary artery spasm is defined as an abnormal contraction of an epicardial coronary artery resulting in myocardial ischemia. Many factors may precipitate coronary artery spasm. Coronary artery spasm frequently occurs at rest, particularly from midnight to early morning. However, in the early morning, even mild exertion may induce coronary spasm. Coronary artery spasm can lead to arrhythmia or rarely sudden death. Coronary spasm is forecast to 3%-4% of patients undergoing diagnostic coronary angiography for chest pain syndromes. A 41-year-old male was admitted to out-patient clinic due to a feeling of tightness in the chest, and dyspnea for 1 month. He have had a history of smoking for ten years. Physical examination on admission, the BP was 140/75 mmHg. Cardiovascular stress test was positive result and coronary angiography was performed. A diffuse filling defect of ∼75% was found in the left anterior descending and cicumflex artery. (Figure 1A), and thus the spasm of this vessels was proposed. Coronary spasm was confirmed by intravascular ultrasound(IVUS). However, the stenosis in the coronary angiography was not observed during IVUS. Immediately, an intracoronary injection of 250 μg of nitroglycerin was done. However, the entire filling defect remained (Figure 1B). Second intracoronary injection of 250 μg of nitroglycerin was done, but spasm hasn’t resolved. Lastly, intracoronary injection of 5 mg diltiazem was done. Coronary artery spasm disappered after intracoronary injection of diltiazem (Figure 1C,D). If the coronary spasm suspected, especially patient is young and absent of coronary risk factors, IVUS and intracoronary drug injection should be performed.