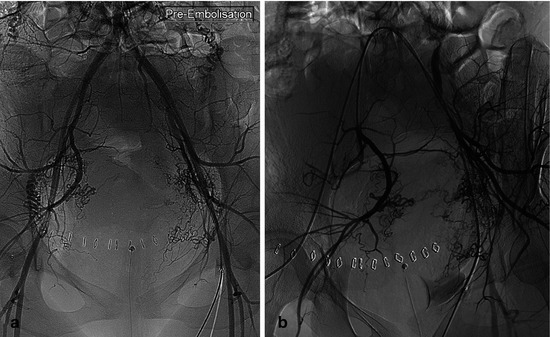
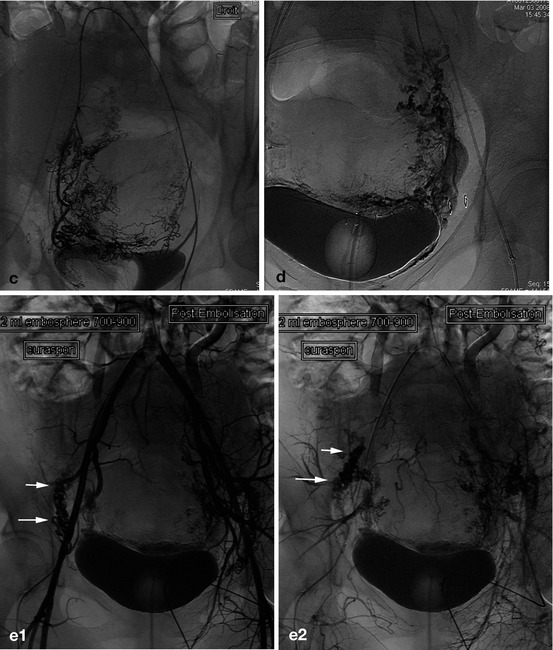
Fig 18.1
Postpartum hemorrhage: uterine arteries in late pregnancy. (a) Selective injection of the left hypogastric artery from a right femoral access (crossover), 27° RPO view. Modal termination of the hypogastric artery: bifurcation in anterior and posterior trunks; note the increased diameter of a very tortuous uterine artery (first branch of the anterior trunk) (arrow), usual in late pregnancy. (b) Injection at the end of the right common iliac artery (from a left femoral puncture: crossover catheterization), 30° RPO view, exposing the iliac bifurcation, before selective catheterization of the anterior trunk of the right hypogastric artery. (c) After selective catheterization of the hypogastric artery, selective injection (25° LPO view), to distinguish the posterior trunk from the uterine artery (a branch of the anterior trunk), often the largest branch in late pregnancy (arrow: ascending path of uterine artery, enlarged in late pregnancy)
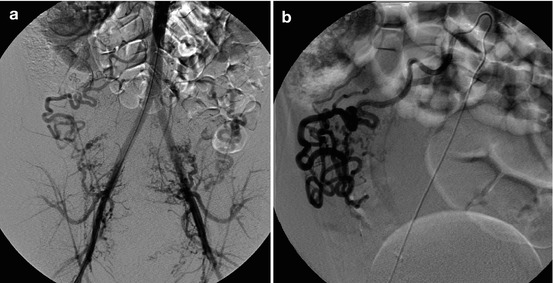
Fig. 18.2
(a) Postpartum hemorrhage, aortography, frontal view: right ovarian artery, arising from the right edge of the infrarenal aorta, enlarged and involved in uterine perfusion. (b) Selective injection before embolization by absorbable gelatin sponge
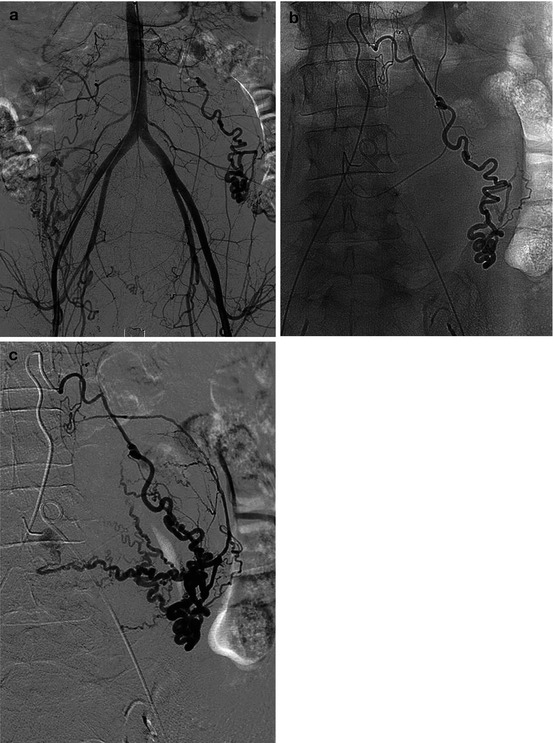
Fig. 18.3
Postpartum hemorrhage: enlarged left ovarian artery involved in the vascularization of an atonic uterus. (a) Aortography. (b, c) Selective catheterization
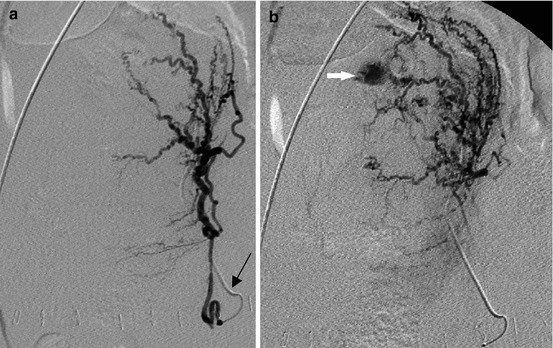
Fig. 18.4
(a) Frontal view, selective injection of the left uterine artery (4 F Cobra catheter) (black arrow) after right femoral puncture followed by a crossover. (b) Hypervascularization of the uterine fundus, with late extravasation (white arrow): PPH caused by uterine atony
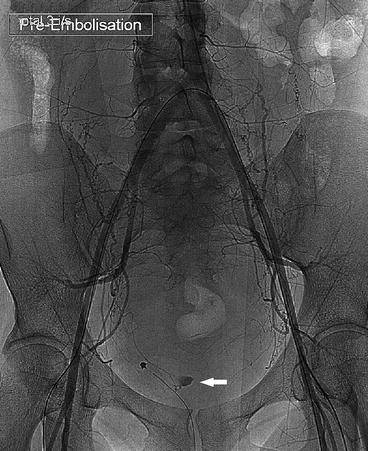
Fig. 18.5
PPH as a complication of a vaginal delivery (twin pregnancy): the bleeding was related to a long straight vaginal wound, easily seen on this aortographic injection (arrow), which will be embolized by gelfoam