Fig. 8.1
68-year-old M, bifocal HCC (2 lesions of 3 cm diameter) on healthy liver; a right hepatectomy has been planned. The hepatic volumetry analysis led to plan a preop right portal branch embolization. (a) CT, arterial phase: segment IV tumor (the second tumor was located in segment VII). (b) Transparietal left portal vein puncture: note the end of the introducer sheath (arrow) and a pigtail catheter in the portal vein trunk. (c) Intermediate control after exclusion of anteromedial segmental branches, using a Histoacryl + Lipiodol emulsion. (d) Last control after exclusion of the posterolateral branches (pigtail catheter in the portal vein)
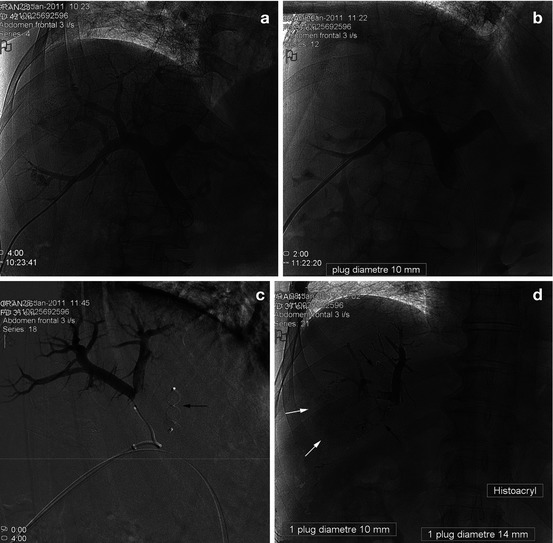
Fig. 8.2
Sgt VI 5 cm HCC, a right lobectomy has been planned, after a TACE session first, and then a portal embolization 2 m later. (a) Transparietal puncture of the right portal vein, decided because the access to the left portal vein was ultrasonically considered too difficult. (b) Control portography after exclusion by AVP of the segment IV portal branch, arising from the right portal vein. Note the security GW beside the introducer sheath in the portal vein. (c) Selective catheterization of the segment VIII branches (Mikaelsson catheter): occlusion with glue (Histoacryl) (arrow: AVP previously delivered in the segment IV branch). (d) Plain film (without any ICM injection) after introducer sheath retrieval: occlusion with an AVP of the posterolateral branch (with this ipsilateral access, a final portography was impossible). Note the spontaneous radio-opacity of Histoacryl-Lipiodol emulsion used to occlude the segment VIII branches; AVP: black arrow; intratumoral retention of Lipiodol, consequence of the previously performed TACE (white arrows)
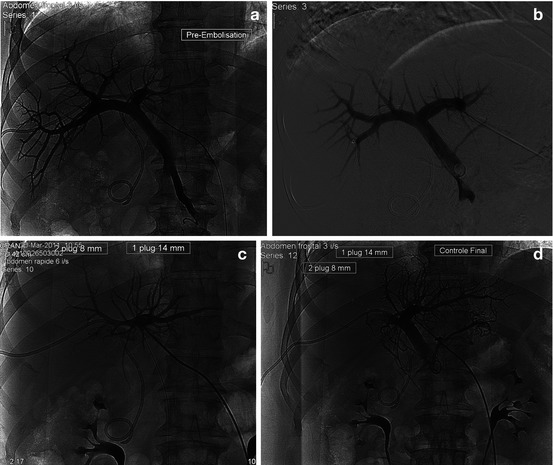
Fig. 8.3
Klatskin 3 B cholangiocarcinoma: a right lobectomy has been decided, preceded by a right portal vein preoperative embolization. An internal–external biliary drain has also been installed. (a, b) After a transparietal left portal vein puncture: portography (frontal (a) and oblique (b) views), via a pigtail catheter in the portal vein. (c) Sheath injection in the left portal branch: occlusion with an AVP of the right lobe branches. Note the remaining GW in the portal vein. (d) Last control portogram, after AVP exclusion of the segmental IV branch
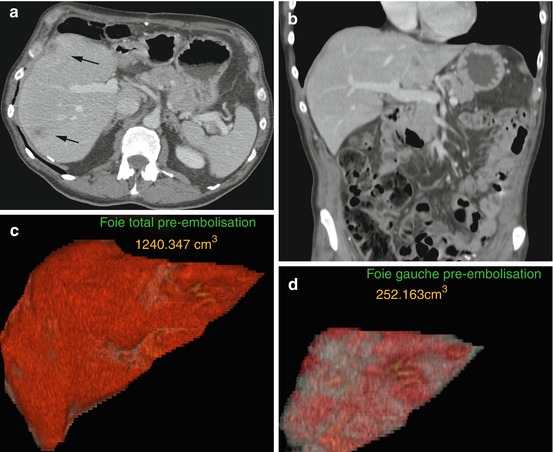
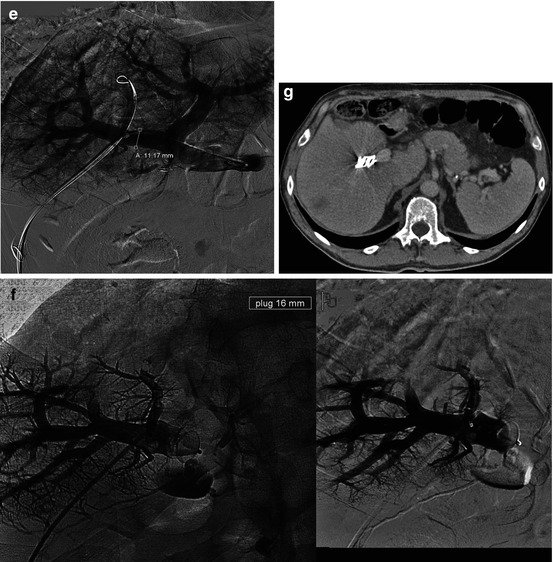
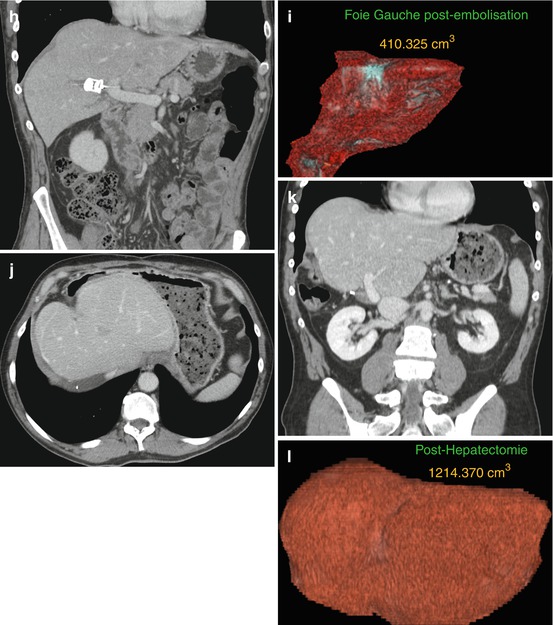
Fig. 8.4
50-year-old W, sigmoid cancer with synchronous liver metastases. First, the following have been performed: a colic resection and preop radiofrequency ablation of left liver metastases. A right hepatectomy is then planned. (a) Pre-embolization CT, portal phase: metastases (arrows). (b–d) CT frontal reconstruction and hepatic volumetry. The volume of the left lobe is limited: FLR is evaluated as 25 % of this healthy liver volume. (e) Transparietal portography (right portal branch access; pigtail catheter in the portal vein, GW in the paramedian sector to guide the AVP release). (f) Control opacification via the introducer sheath after the release of a 16 mm diameter AVP in the right portal vein. (g–i) CT 3 w later: correct position of the plug in the right portal vein; more than 50 % induced liver hypertrophy. (j–l) CT 6 m after right hepatectomy
References
1.
Perarnau JM, et al. Transjugular preoperative portal embolization (TJPE) a pilot study. Hepatogastroenterology. 2003;50(51):610–3.PubMed
2.
Tsuge H, et al. Right portal embolization before extended right hepatectomy using laparoscopic catheterization of the ileocolic vein: a prospective study. Surg Laparosc Endosc. 1994;4(4):258–63.PubMed
3.
Gibo M, et al. Percutaneous ipsilateral portal vein embolization using a modified four-lumen balloon catheter with fibrin glue: initial clinical experience. Radiat Med. 2007;25(4):164–72.PubMedCrossRef
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


