Fig. 60.1
CT scan of mesothelioma on the right side. The right lung is surrounded by pleural tumour, and the middle and lower lobe are compressed by pleural effusion
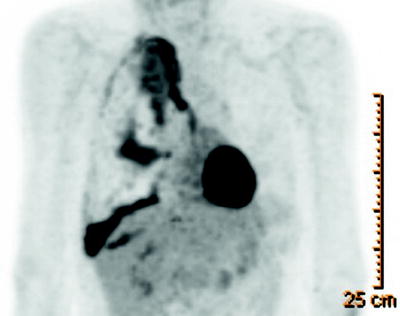
Fig. 60.2
PET scan of the same patient, showing enhanced uptake of the pleura, especially at the level of the mediastinum and pleura
Talc is a mineral in its pure form and is defined as hydrated magnesium silicate. Pure talc does not exist; it is mined throughout the world in open pits. Depending on the deposit were talc is found, it is contaminated with associated minerals like chloride (magnesium and aluminium silicate) and calcite (calcium carbonate). Because of the different geologic circumstances of talc formation, ever talc deposit is unique in morphology, varying from highly lamellar tot compact.
Talc and Asbestos
In the past, there was some concern that intrapleural talc could lead to mesothelioma due to asbestos contamination. The association of talc and asbestos is mainly based on overly broad definition of asbestos and non-specific analytical techniques. The geologic conditions under which talc and asbestos form are dissimilar. Besides, the manufacturer of talc confirms that the product is free of asbestos contamination by X-ray diffraction or infrared spectrophotometry.
There is no ground for any fear of asbestos contamination of medical talc; long-term follow-up studies after talc pleurodesis never showed mesothelioma or an increased incidence of other pleural malignancy.
Safety of Talc Pleurodesis: Relation to Particle Size
After incidental reports of early complication after talc pleurodesis, most important ARDS with sometimes fatal outcome, doubts rose about the safety of intrapleural instillation of talc. Despite these concerns, talc was widely used for pleurodesis, and large series including a total of almost 1,000 patients reported no complications after talc pleurodesis.
In experimental studies, the relation between small size of talc particles and inflammation or necrosis of the lung parenchyma was demonstrated. In a clinical study, a relation was demonstrated between pulmonary inflammation and small talc particle size. Increased lung inflammation was found after small particle size talc pleurodesis.
In a prospective cohort study including 558 patients in 14 centres in 11 countries, talc pleurodesis for malignant pleural effusion was performed with exclusive use of large particle size talc (of French origin). No ARDS or other severe complications were found in this study. After talc poudrage, a slight increase in oxygen supply, which was significant during the first 48 h after thoracoscopy, was noticed. Besides, a slight but significant rise of temperature was found in the first 4 days after thoracoscopy and talc poudrage.
Both side effects were clinically insignificant, and the use of large particle size talc for malignant pleural effusion has been considered as safe since the outcome of this study.
All clinicians performing pleurodesis should have knowledge of the particle size of the talc they use. Small particle size talc or medical talc without known particle size should not be used for pleurodesis in humans.
Alternative Agents for Chemical Pleurodesis
Bleomycin
Bleomycin is an anti-neoplastic agent, but its mechanism of action after intrapleural installation is predominantly as a chemical sclerosant. After systemic absorption, its systemic side effect as an anti-neoplastic agent (myelosuppression) is minimal. The technique of bleomycin application is intrapleural installation of a solution of 60,000 IE in saline. The success rate of bleomycin is around 60% in malignant pleural effusion, which is inferior to results obtained with talc. Depending on patent regulations, bleomycin is expensive in some countries.
Tetracycline and Doxycycline
Tetracycline used to be a popular agent for chemical pleurodesis, until production ceased in many countries. The results of tetracycline pleurodesis was slightly inferior to talc. Doxycycline has been tried as an alternative. The efficacy of doxycycline for pleurodesis has been demonstrated in animal studies. However, severe local effects were found. The availability of clinical data with doxycycline pleurodesis in humans is limited. A randomised trial to compare the efficiency of talc powder and doxycycline for pleurodesis in malignant pleural effusion was terminated prematurely, because an interim analysis showed a highly significant difference in favour of talc. Besides, severe respiratory failure in response to doxycycline pleurodesis has been described. The place of doxycycline as an alternative chemical agent for pleurodesis is therefore limited.
Iodopovidone
Iodopovidone is a topical antiseptic. It has been reported as a promising pleurodesis agent, but its mechanism of action is unknown. In a recent study with small numbers of patients, it has shown to be equally effective to talc. Previous studies showed high success rate of 90%. The pleurodesis solution consisted of a mixture of 20 ml 10% iodopovidone and 80 ml normal saline solution. The major side effect was intense pleuritic pain, accompanied by systemic hypotension in 6% of patients. Severe complications were not observed. The advantage of iodopovidone is the wide availability and the low costs.
Silver Nitrate
In a small prospective study, silver nitrate appeared to be equally effective to talc for producing a pleurodesis. Twenty millilitres of 0.5% silver nitrate was injected in the chest tube. There was no difference in pain score between silver nitrate and talc. Silver nitrate is widely available and inexpensive. Most significantly, side effects have been described, but clinical studies with a large number of patients and long-term follow-up are not available.
Talc Pleurodesis: Poudrage or Slurry?
Talc has been accepted as the most effective sclerotic agent in pleurodesis. There are two different techniques of intrapleural administration:
1.
Insufflation of dry talc powder into the chest cavity during thoracoscopy, after complete removal of pleural fluid. This treatment is performed in the operation room, under local or general anaesthesia. The advantage of this technique is the combination with the diagnostic thoracoscopy, during which the pleural biopsies can be obtained to assess the specific diagnosis of malignant disease.
2.
The other technique is administration of talc slurry (a suspension of talc powder in saline) through a chest tube, after removal of all, or at least as much as possible pleural fluid, and complete re-expansion of the lung confirmed by chest X-ray. This procedure can be performed at the bedside.
Which of these two techniques provides the best results in talc pleurodesis?
Several studies have addressed this issue in the past decade. In a small-randomised study, no significant difference in recurrence rate was found between talc poudrage and talc slurry. In a porcine study, talc poudrage was performed in one hemothorax and talc slurry in the other in 21 pigs. The animals were sacrificed after 30 days, and both density and distribution of adhesions were scored. Talc poudrage and talc slurry appeared to be equally effective for both density and distribution of adhesions.
A large, prospective randomised trial was published in 2005. Of 501 patients, 242 were randomised to talc poudrage and 240 to talc slurry. The rate of successful pleurodesis after 30 days was equal in both groups, 78% in the talc poudrage group versus 71% in the talc slurry group. However, talc poudrage appeared to be more efficient in the subgroup of breast and lung cancer patients, with a success rate of 82% versus 67% for talc slurry.
In a small, prospective non-randomised study, it was shown that poudrage was significantly more successful than slurry. Successful pleurodesis was immediately obtained in 87.5% of the talc poudrage group, versus 73% in the talc slurry group. Lifelong pleural symphysis was obtained in 82% in the talc poudrage group and 62% in the talc slurry group. In a retrospective study comparing VATS pleurodesis and chest tube pleurodesis in 138 patients, it was found that the recurrence-free survival after VATS was significantly longer than after chest tube pleurodesis. The interpretation of these results is not obvious, as during the VATS procedure both mechanical and chemical pleurodesis was used, and for chest tube pleurodesis not only talc was used but also tetracycline and other mechanical pleurodesis agents.
Unidirectional conclusions and recommendations are not easy to draw from the studies. Talc poudrage seems to be more effective in pleural metastasis in lung and breast cancer, which together represent the majority of patients with malignant pleural effusion. If a diagnostic thoracoscopy is performed for pleural effusion, talc pleurodesis should be performed in case of a malignant appearance of the pleura as the circumstances for pleurodesis after removal of the pleural fluids under visual guidance are optimal.
Talc Pleurodesis Versus Outpatient Treatment with Tunnelled Pleural Catheters
Because of its proven efficacy, talc pleurodesis is the accepted gold standard for treatment of malignant pleural effusion. Outpatient treatment with a permanent tunnelled pleural catheter is reserved for patients with recurrence after chemical pleurodesis, mostly due to trapped lung. In patients with a low performance score and limited life expectancy, a tunnelled pleural catheter may be the treatment option of first choice.
Some authors have suggested a tunnelled pleural catheter as a first-line treatment option for pleurodesis in malignant pleural effusion, under the condition of existing expertise and facilities of outpatient management, because of the high success rate and the limited rate of complications. Tunnelled pleural catheters can be inserted in an outpatient setting under local anaesthesia. Pleural fluid is drained via vacuum bottles in a home-based setting, on a regular or as needed basis. In patients with indwelling pleural catheters, spontaneous pleurodesis may occur, with the recorded success rate of more than 40% in several studies. Recurrence of malignant pleural effusion requiring a repeated invasive procedure is limited less than 9% according to the largest published study of 250 patients. The downside of treatment of malignant pleural effusion with tunnelled pleural catheter is the costs: the vacuum bottles need to be replaced frequently and are expensive. Moreover, in some European countries the vacuum bottles are not reimbursed by health insurance companies. In these cases, the vacuum bottles may be replaced be urinary bags, although there are no published data about the efficacy.
In a recent American study, cost data for PleuRX® and talc treatment were compared using Medicare reimbursement data. Talc pleurodesis appeared to be less costly than PleuRX® treatment, with similar effectiveness. PleuRX® treatment became more effective when life expectancy was 6 weeks or less. Due to the lack of prospective randomised studies, the question, if a tunnelled pleural catheter is equally effective as talc pleurodesis and consequently can serve as a first-line treatment option in malignant pleural effusion, is still unresolved. Pleural-tunnelled catheter is maybe the treatment of first choice in patients with limited life expectancy and may serve as an alternative treatment in case of failure of talc pleurodesis or trapped lung. Besides, local expertise, like the ability to perform thoracoscopy and facilities for home-based care, may influence the optimal choice for treatment with malignant pleural effusion.
Mechanical Pleurodesis
Mechanical pleurodesis is obtained by rubbing of the pleura (abrasion) or removal of the parietal pleura (pleurectomy). Both techniques are invasive surgical procedures and are much less frequently performed than chemical pleurodesis. In an experimental study in dogs, talc poudrage and mechanical abrasion proved to be effective, and pleurodesis results were superior to Nd-YAG laser or argon beam coagulation. In another experimental study, talc (both slurry and poudrage) was superior to abrasion. Two abrasion techniques were used: mechanical abrasion with a dedicated pleural abrader and focal gauze abrasion by limited thoracotomy. The results of the pleural abrader were unsatisfactory; hardly any pleurodesis was found at autopsy after 30 days. Results of focal gauze abrasion after thoracotomy were better, equal to talc slurry but inferior to talc poudrage.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


