Pleural Mass
Jonathan H. Chung, MD
DIFFERENTIAL DIAGNOSIS
Common
Pleural Pseudotumor
Pleural Plaque
Pleural Thickening
Empyema
Rounded Atelectasis
Subpleural Lung Cancer
Less Common
Pleural Metastasis
Pulmonary Infarctions (Subpleural)
Extrapleural Abnormality
Benign or Malignant Chest Wall Mass
Extrapleural Hematoma
Fracture
Pleurodesis
Rare but Important
Lymphoma
Malignant Mesothelioma
Fibrous Tumor of Pleura
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Pleural vs. subpleural (pulmonary)
Pleural: Obtuse margins with chest wall, well-defined margins with lung, no air bronchograms
Subpleural (pulmonary): Acute margins with chest wall, ill-defined margins with lung, air bronchograms
Differentiation of extrapleural vs. pleural abnormality can be difficult
Extrapleural component present if concomitant effect on extrapleural structures
Rib destruction in extrapleural tumor
Extension of mass into chest wall on CT
Internal displacement of extrapleural fat
Incomplete border sign on radiograph highly suggestive of extrapulmonary (pleural or extrapleural) lesion
Margins partially sharp and partially unsharp
Helpful Clues for Common Diagnoses
Pleural Pseudotumor
Loculated pleural fluid in interlobar fissure, usually minor fissure
History of congestive heart failure
Oval shape, peripheral tapering along margins of pseudotumor
Pleural Plaque
Related to previous asbestos exposure
Bilateral focal regions of pleural thickening, ± calcification, often symmetric
Posterolateral, diaphragmatic, and pericardial preponderance; sparing of apices and costophrenic angles
Pleural Thickening
Related to asbestos exposure, previous infection or inflammation, hemothorax
Usually smooth thickening of pleura, often diffuse, ± foci of calcification
May affect costophrenic angles; often broad extension as opposed to focality of pleural plaques
Empyema
Pus in pleural space; most often from pneumonia/pulmonary abscess
Loculation, split pleura sign
Lenticular shape
Nondependent location
Rounded Atelectasis
Definitive diagnosis on CT requires 4 findings
Pleural thickening, pleural effusion, or pleural plaque
Broad-based intimate attachment of mass-like consolidation to pleural abnormality
Volume loss
Comet tail (or hurricane) sign: Swirling of bronchovasculature into mass-like consolidation
Subpleural Lung Cancer
Most common in upper lung zone (2/3 of primary lung cancers)
Spiculated margins, pleural tail, thick-walled cavitation
Hilar and mediastinal lymphadenopathy
Helpful Clues for Less Common Diagnoses
Pleural Metastasis
Adenocarcinoma most common; drop metastases from invasive thymoma
Unexplained unilateral pleural effusion, irregular pleural thickening, and nodules ± enhancement
Pulmonary Infarctions (Subpleural)
Most often from pulmonary arterial embolism
Usually in setting of superimposed cardiac dysfunction (cardiomyopathy, congestive heart failure)
Both pulmonary and bronchial arterial supply to lung reduced
Lower lung predominant, peripheral/subpleural, wedge-shaped consolidation
Resolves over months (retains its original shape) rather than patchy resolution as in pneumonia
Extrapleural Abnormality
Mass effect on or destruction of extrapleural structures
Extrapleural hematoma
High association with rib fractures and elderly patients; sequela of blunt or penetrating trauma
Localized hyperdense fluid collection often internally displacing extrapleural fat stripe
Biconvex shape suggests arterial injury (usually intercostal)
Pleurodesis
Iatrogenic fusion of visceral and parietal pleura; talc most often used
Treatment of recurrent pleural effusion (most often malignant etiology)
Unilateral high density foci, most often dependent
Associated pleural thickening (which can be nodular) or loculated pleural fluid
Helpful Clues for Rare Diagnoses
Lymphoma
Concomitant mediastinal lymphadenopathy; ± pleural effusion
Can be difficult to differentiate pleural from extrapleural involvement
Malignant Mesothelioma
Stigmata of previous asbestos exposure: Pleural plaques, pleural thickening, pleural effusion
Lobulated pleural thickening; small hemithorax
CT findings that suggest malignant pleural disease (mesothelioma or metastases)
Circumferential involvement of pleura, including visceral pleura
Involvement of mediastinal aspect of pleura
Nodularity
Thickness greater than 1 cm
Fibrous Tumor of Pleura
Well-marginated, large pleural mass with avid enhancement (may be heterogeneous in larger tumors)
Margins with chest wall may be acute in large tumors
Majority arise from visceral pleura; up to half pedunculated; may be mobile
Image Gallery
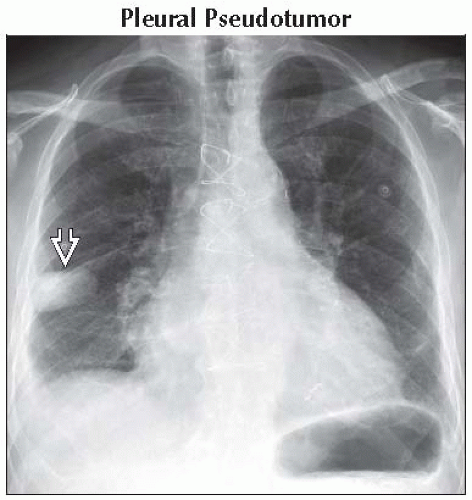 Frontal radiograph shows an oval mass  in the peripheral mid right lung in this patient with cardiomegaly and history of heart failure. in the peripheral mid right lung in this patient with cardiomegaly and history of heart failure. |
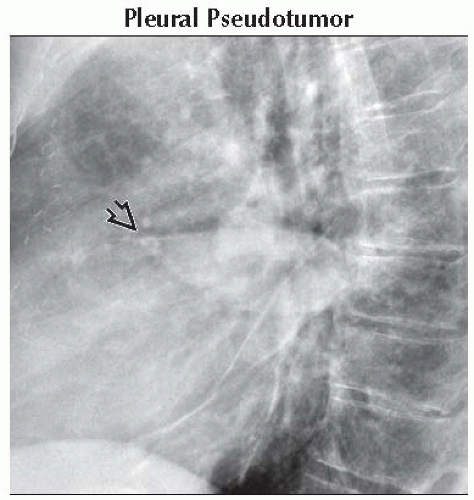 Lateral radiograph shows that the mass is located along the minor fissure and has tapered anterior and posterior margins (best seen anteriorly  ). These findings are most consistent with a loculated pleural fluid collection. ). These findings are most consistent with a loculated pleural fluid collection. |
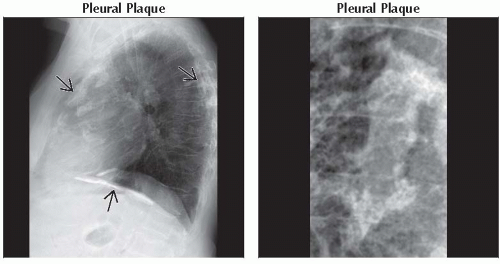 (Left) Lateral radiograph shows calcified pleural plaques
 along the anterior, posterior, and diaphragmatic aspects of the pleura. (Right) Frontal radiograph (magnified) shows the typical “holly leaf” appearance of an en face calcified pleural plaque on the anterior pleural surface. along the anterior, posterior, and diaphragmatic aspects of the pleura. (Right) Frontal radiograph (magnified) shows the typical “holly leaf” appearance of an en face calcified pleural plaque on the anterior pleural surface.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|