19 Pleural Effusions of Other Origin
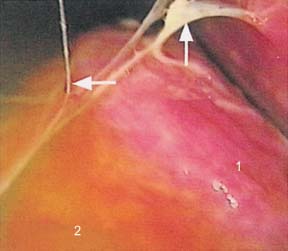
Fig. 19.1
Complicated parapneumonic effusion. The lung (1) is bathed in turbid fluid (2) and fibrinous adhesions (→).

Fig. 19.2
Fibrinopurulent stage of empyema. The photograph shows the fluid collection and fibrin, creating adhesions and loculations.
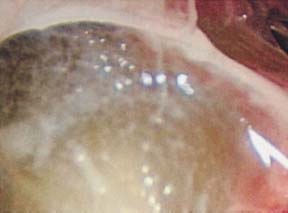
Fig. 19.3
Fibrinopurulent stage of empyema. The photograph shows fibrin adhesions and the formation of a loculation, filled with empyema fluid.

Fig. 19.4
Nonspecific pleural effusion with adenovirus infection. After pneumothorax induction, there was only minimal effusion. The right upper lobe was adherent dorsally. The lower lobe (1) and middle lobe (2) look normal; the interlobar septum was displaced by a flat, nonvascularized wide adhesion. Additional adhesions are present between the lower lobe and the diaphragm (3), which appears brownish through the remaining effusion.
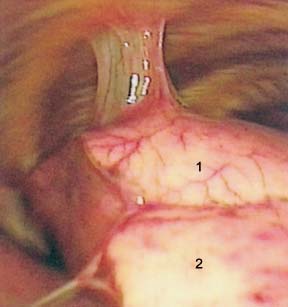
Fig. 19.5
Nonspecific pleuritis with pleuropulmonary adhesions. The picture shows the right lower lobe (1) attached to the chest wall by a broad adhesion and the base of the middle lobe (2) with an adhesion toward the diaphragm.

Fig. 19.6
Nonspecific pleuritis with pleuropulmonary adhesion. The picture shows a broad adhesion between lung and chest wall.

Fig. 19.7
Pleural effusion associated with pulmonary infarct. After drainage of 300 mL of amber effusion: a normal left upper lobe (1). The edge of the lower lobe (2) shows some bloody effusion on its surface. In the underlying, subapical lower lobe segment is seen a bandlike, firm hemorrhagic infarct (3) adjacent to the somewhat hyperemic lateral basal segment (4). Intersegmental septum (→).
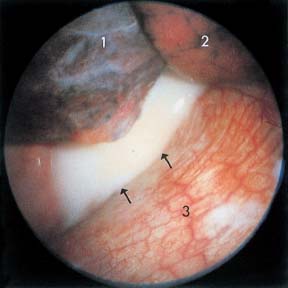
Fig. 19.8
Idiopathic chylothorax. After drainage of 2100 mL of chylous pleural effusion, the upper lobe and lower lobe (1) are atelectatic; the middle lobe (2) is well ventilated. Parietal pleura and diaphragm (3) are not inflamed and have normal vascularity. From the inter-lobar septum, a chylous stream flows (→).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


