Chapter 5
Peripherally Inserted Central Catheters and Ports
PERIPHERALLY INSERTED CENTRAL CATHETERS
Venous Anatomy
A review of the upper extremity venous anatomy will be helpful before discussing peripherally inserted central catheters (PICCs) and subcutaneous arm ports. In the upper extremity, there are superficial and deep veins. The superficial veins are the basilic vein, cephalic vein, and median cubital vein. The main deep veins correspond to the arteries, including the radial, ulnar, and interosseous veins in the forearm; the brachial veins in the arm; and the axillary vein in the axilla. In the upper extremity, the superficial veins are important for catheter or port placement. In the arm, the sites most often used for peripheral line placement are, from medial to lateral, the basilic vein, the brachial veins, and the cephalic vein. The basilic vein is relatively superficial and usually is the largest in the arm. Because of these two anatomic facts, the basilic vein is the optimal site for PICC or port insertion. The puncture of the basilic vein is easy because of its caliber and its shallow location under the skin. Furthermore, because the luminal diameter is larger, the rate of catheterrelated thrombosis is low.
The brachial veins often are paired and located deep in the soft tissue, adjacent to the brachial artery and in close proximity to the median nerve. Therefore, the brachial veins are less desirable than the basilic vein for PICC insertion. The deep location can lead to catheter kinking if the angle of puncture and catheter introduction is too steep. Furthermore, if the operator does not palpate the brachial artery while using contrast-guided fluoroscopy for venipuncture, one could inadvertently puncture the unopacified artery as the needle travels to enter the brachial vein; however, the brachial veins still may be a good location for PICC insertion. Ultrasound-guided puncture of the brachial veins allows direct visualization of the brachial artery to ensure that the artery is not traversed during puncture.
The cephalic vein is located lateral in the arm and is also superficial. The cephalic vein courses over the biceps muscle and may make an acute caudal turn at the shoulder as it enters the axillary vein in the deep pectoral groove. The location of the cephalic vein over the biceps muscle may result in excessive movement of the catheter during arm flexion and extension, causing discomfort and limiting arm motion as well as kinking of the catheter. In addition, the caudal turn at the shoulder may result in the catheter entering the axillary vein in a peripheral direction rather than centrally during insertion. This may be a problem during insertion without fluoroscopy and may be time consuming and require additional manipulation to redirect the catheter into the superior vena cava (SVC). The cephalic vein is also the smallest of the arm veins; therefore, a greater incidence of thrombosis can be expected after PICC insertion.
Additional factors to consider in selecting the optimal insertion site include the presence of acute or chronic thrombus in the target vein, soft-tissue inflammation, induration or hematoma from prior intravenous (IV) sites, or failed IV placements. Overall, the basilic vein is the optimal site for PICC, followed by the brachial veins and the cephalic vein. If the patient has chronic renal insufficiency and is a candidate for an upper-extremity graft or an arteriovenous fistula, PICC lines should be avoided.
Indications and Contraindications
The primary indication for PICC placement is short- to intermediate-term central venous access, that is, from approximately 2 to 8 weeks. PICCs are used for antibiotic therapy, hyperalimentation (total parenteral nutrition, or TPN), chemotherapy, fluid administration, and pain-control medication administration. Important considerations prior to PICC placement are the duration of therapy, type of medication (viscosity), frequency of administration, and number of medications needed. Insight into these questions mandates proper selection of either a single- or dual-lumen catheter, thus keeping the patient and physician well served by the venous access service. If questions arise concerning the clinical need or application of the PICC, a brief discussion with the referring physician often clarifies issues and saves headaches.1,2
In general, PICCs have optimal application in the 2- to 8-week period. Some PICCs, however, last much longer, up to a year, with meticulous care.
Dual-lumen PICCs are used in cases where multiple drugs or simultaneous infusions are needed. Single-lumen PICCs allow greater flow rates than dual-lumen PICCs because of their larger inner lumen and thus are preferred for hyperalimentation (TPN) or more viscous infusions. The Poiseuille law states that the flow rate is directly proportional to the fourth power of the radius and inversely proportional to the viscosity of the fluid infused as well as to the length of the catheter. Hence, the greatest flow rates will be achieved in the catheter with the largest luminal diameter (single-lumen PICCs), shortest length, and least viscous infusate. Unfortunately, a catheter intended for infusion of TPN should have a lumen dedicated only to TPN and should not be used for other infusions or blood draws. Therefore, if a single-lumen catheter is placed for TPN, other venous access often is required.3
The PICCs have significant advantages over short-term centrally placed catheters because there is no risk of pneumothorax and very little risk of bleeding, even in thrombocytopenic patients or patients taking anticoagulants. In addition, PICC insertion success rates are higher than 98%; they are cost effective, practical, and avoid considerable pain and discomfort for patients with poor peripheral veins in whom multiple punctures may be needed to start an IV which will last only several days.1,2 Furthermore, many chemotherapeutic agents are irritant or caustic to peripheral veins and therefore are better tolerated if given centrally. Patients needing relatively short duration of treatment do not require placement of a longer-term tunneled catheter. PICCs also may have a lower incidence of central venous stenosis relating to central catheters because of the small diameter of the catheter and because an axillary or subclavian vein puncture is not needed.
Contraindications to PICC insertion include phlebitis or cellulitis at the insertion site. A relative contraindication may include central venous stenosis or occlusion. In such cases, the contralateral arm can be used for insertion, or the PICC may be placed to the SVC via a collateral vein using a 0.018-inch hydrophilic wire to negotiate the venous channels and advance the catheter into the right atrium (RA). Other relative contraindications may include a prior mastectomy on the side of planned insertion or that a dialysis graft or arteriovenous (AV) fistula might be needed in the future in the arm.
Insertion Techniques
It is essential that the patient’s medical record be reviewed before the procedure is performed to ensure that a PICC, rather than other central catheters, is the optimal choice for central venous access. As discussed already, the duration of the therapy must be short to intermediate in length (2 to 8 weeks) for PICC placement. Otherwise, a tunneled catheter or port is better if the patient is likely to have a repeated and long-term need for venous access (e.g., cystic fibrosis, human immunodeficiency virus). Also, a review of the medications and dosing regimen is important to determine whether multiple simultaneous infusions will require a dual-lumen PICC or whether a single lumen will suffice. This review should include knowing what is going to be infused through the catheter. Hyperalimentation (TPN) is more viscous than saline. The more viscous the infusate, the larger the lumen needed; so a single-lumen catheter may be preferable. If the fluids to be infused are caustic, such as chemotherapeutic agents, the tip placement needs to be in the high-flow SVC or the RA. If only saline is to be given, it will be tolerated easily in a more peripheral position of the catheter tip. A prior history of allergic-like reaction to radiographic contrast material necessitates placement of the PICC using CO2 or ultrasound guidance. On occasion gadolinium can be used as a contrast agent. A brief review of operative and progress notes for prior central catheter placements, cardiac pacer placement, or a known history of central venous stenosis or thrombosis will avoid confusion or embarrassment and allow choosing the best arm for insertion.
After a quick chart review, we inspect the patient’s chest and arms. If a prior subclavian catheter insertion site is discovered, the ipsilateral arm should be avoided because of the risk of subclavian stenosis. Also, chest-wall vein collaterals may be present on one side as warning signs of subclavian or brachiocephalic vein occlusion. We also examine the arms for phlebitis or cellulitis from prior IV sites or infiltrated IVs. If no adverse conditions exist in either arm, the nondominant arm is preferable for placement of PICC.
Several techniques for PICC insertion are effective. These include fluoroscopically guided venous puncture using iodinated contrast material or CO2, ultrasound-guided venous access with fluoroscopic insertion, or bedside insertion, which requires taking a chest radiograph to check tip position. In our experience, fluoroscopic venous puncture with contrast material is quicker than ultrasound guidance and also allows visualization of most of the veins and thus the opportunity to choose the optimal vein and site for insertion. Therefore, this technique is discussed in greatest detail.
A 22-gauge IV is started in a forearm, wrist, or hand vein. A 23- or 25-gauge butterfly needle can be used if the veins are not suitable for cannulation with an Angiocath. The practice of injecting a contrast agent through a butterfly needle should be discouraged, however, because of the increased risk of infiltration. The initial contrast injection should be performed under fluoroscopic control while observing the needle to ensure that the contrast is not extravasating. In our opinion, if an Angiocath cannot be placed, the next best option is to place the PICC under sonographic guidance rather than to place a butterfly needle for contrast injection. The IV is connected to extension tubing, which will allow injection of contrast material without disrupting the sterile field. The location of the port for the IV tubing should be planned in advance, prior to preparing the sterile field, so that a last-minute search for the port under the sterile field will not be necessary.
The patient is placed on the angiographic table with the arm abducted, resting on an arm board. The image intensifier is positioned over the midarm so the insertion site is visualized as well as the shoulder and chest when the table is moved. The arm then is raised and held by the circulating nurse and is prepped from axilla to below the elbow with 2% Chlorhexidine or Betadine solution (Purdue, Fredrick, Norwalk, CT). The entire circumference of the arm should be painted from the axilla to below the elbow with each sponge, and the axilla should be painted last with each sponge. This process of painting the arm and the axilla should be repeated three times. Sterile towels (or a sterile sheet) are placed under the prepped arm, and a sterile tourniquet is placed as high as possible on the arm. The arm then is lowered with the palm of the hand supinated to expose the medial aspect of the arm. The basilic vein is optimally exposed for puncture with the arm in this position. The distal arm and hand are covered with sterile towels, as are the axilla and chest region. A sterile angiography drape is placed over the patient’s body with a sterile image-intensifier cover placed as well. This leaves the upper arm uncovered for the procedure. The junction of the proximal and midhumeral region is placed under the image intensifier, and iodinated contrast material or CO2 is injected by the circulating nurse to opacify the basilic, brachial, and cephalic veins. It is helpful to compress the forearm gently to “pump” contrast material from the forearm to the arm, giving more complete opacification of the arm veins.
HELPFUL HINTS
Do not tie the tourniquet until the vein has been opacified. Perform fluoroscopy while contrast is injected. When the veins are opacified, step off of fluoroscopy, tie the tourniquet, pick up the needle, and then resume fluoroscopy. Continue the slow injection of contrast during this process. This method allows better opacification of the vein because the unopacified blood is pushed out of the vein before the tourniquet is tied. This method also decreases the pressure within the vein and probably decreases the amount of extravasation into the surrounding soft tissues. If the tourniquet is tied before contrast injection, unopacified blood becomes “trapped” in the vein; as iodinated contrast is forcefully injected until there is enough mixing of opacified blood with unopacified blood to visualize the vein, the pressure within the vein is increased to a point that any puncture in the vein—even a single wall puncture—may result in extravasation of contrast.
A 21-gauge, 4-cm-long needle is used to perform a single wall puncture of the basilic vein at the junction of the proximal third and middle third of the arm. It is helpful to magnify the image—even to an extreme level—when attempting to puncture the vein under fluoroscopic guidance (Fig. 5–1). Precise positioning of the needle is easier when the target appears larger. Also, the collimators should be closed so that the needle tip is in the field of view but not the hand holding the needle (Fig. 5–2A). The needle is guided exactly parallel to the basilic vein at approximately a 30- to 45- degree angle and advanced under fluoroscopic observation as it enters the anterior wall of the vein. As discussed in Chapter 3, “Techniques of Venous Catheter Placement,” always puncture the skin directly over the vein with the entire needle superimposed over the vein (on a parallel course over the vein) (Fig. 5–2B). The hand used to perform the venous puncture must be in a stable position, not floating and wagging in the air. With the forearm and wrist resting on the patient’s forearm, the needle should be held like a pencil. The needle tip will indent the vein wall as it enters the lumen. The needle is advanced slowly until the needle tip is seen to compress the vein. The contrast material actually will be seen clearing out from the needle tip as the needle compresses the anterior and posterior walls of the vein together (Fig. 5–2C). A slight forward jab of the needle usually results in puncture of the anterior wall of the vein. The vein should be punctured in the midline to facilitate passage of a 0.018-inch guidewire, which then is advanced to the level of the subclavian vein. With the tourniquet tied, the pressure within the vein is great enough that blood will return through the needle and constant aspiration with a 5 mL syringe is not necessary. If imaging indicates that the needle has entered the vein but no “flashback” is seen, then the syringe should be connected and aspirated while slowly withdrawing the needle.
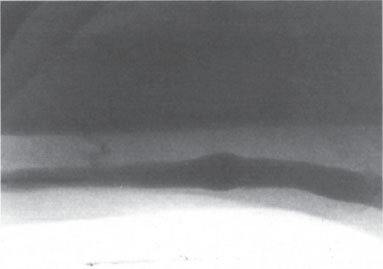
Figure 5–1 Venographic guidance. The field is maximally magnified to give optimal visualization of the vein. The field of view is centered so that the needle is seen, but the operator’s hand is out of the field. The needle is parallel and perfectly superimposed over the vein.



