considered high-risk for surgical revascularization and would have been excluded from the original trials. Indeed, by analyzing the Medicare data from the years when these trials were performed (1992-1993), those treated in the trial hospitals outside of the research protocol and those treated in non-trial hospitals had much higher mortality rates than those treated within the clinical trial protocol (9).
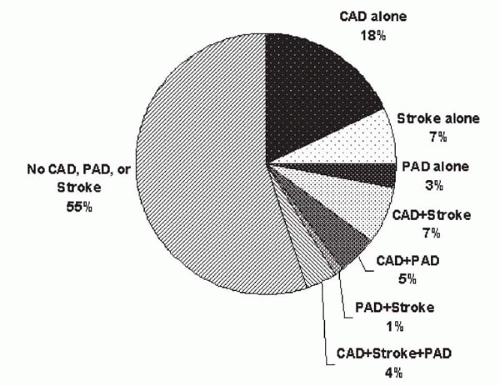 Figure 20.1. High prevalence of multisystemic atherosclerosis identified among 1,802 patients participating in an academic hospital-based geriatric practice. (Reprinted with permission from Ness J, Aronow WS. Prevalence of coexistence of coronary artery disease, ischemic stroke, and peripheral arterial disease in older persons, mean age 80 years, in an academic hospital-based geriatrics practice. J Am Geriatr Soc 1999;47:1255-1256.) |
plaque rupture by balloon, platelet activation, thrombus formation, and spasm of distal arterioles may lead to stroke during carotid intervention (15). Using transcranial Doppler technique during percutaneous carotid intervention, microembolism is detectable throughout the procedure, beginning from catheter placement, but balloon dilatation and stent deployment are responsible for most of the signals detected (16,17). Over the past several years, a number of EPDs have become available in clinical practice or within the context of clinical investigations (Fig. 20.2). Current EPDs can be classified according to three fundamental designs:
TABLE 20.1. HIGH-SURGICAL RISK CRITERIA FOR EXTRACRANIAL CAROTID ARTERY REVASCULARIZATION | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
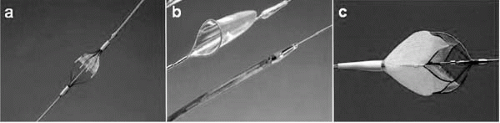 Figure 20.2. Examples of various filter emboli protection devices: (A) Angioguard, (B) EPI FilterWire, (C) Accunet. |
Flow-through filter (Angioguard [Cordis, Warren, New Jersey], Accunet [Guidant, Santa Clara, California], FilterWire EX [Boston Scientific, Santa Clara, California], and NeuroShield [MedNova, Redwood City, California])
Balloon occlusion GuardWire (Medtronic, Minneapolis)
Flow reversal with proximal balloon occlusion (Parodi Anti-Embolism System [ArteriA Medical Science Inc., San Francisco])
TABLE 20.2. PROS AND CONS OF THE USE OF EMBOLI PROTECTION DEVICE DURING CAROTID INTERVENTIONS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
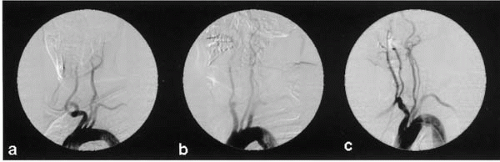 Figure 20.3. Various types of aortic arches and their relationships with the great vessels leading to various levels of challenges for carotid stenting procedure. Selective carotid angiogram on (A) and (B) can be performed with a right Judkins or Bernstein catheter, whereas (C) usually requires reversed curve Newton, Vitek, or Simmons catheters. |
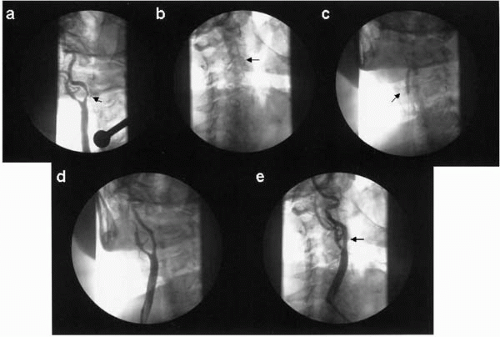 Figure 20.4. A 70-year-old woman suffered from right hemispheric stroke 1 month ago but had full neurological recovery. Magnetic resonance imaging showed a water-shed infarct zone in the corresponding hemisphere, suggestive of high risk for future event. (A) Angiogram confirmed the ultrasound diagnosis of a severe focal stenosis in the right internal carotid artery (arrow). (B) A FilterWire (arrow) was used to cross the lesion. (C) Balloon predilatation. (D) Angiogram after balloon dilatation. (E) Final angiogram after stent placement (Wallstent 7 × 30 mm, arrow). |
Anticoagulation using unfractionated heparin (activated clotting time 250 to 300 seconds) or bivalirudin is then provided. An EPD (e.g., FilterWire, Angioguard, GuardWire) then is advanced across the lesion and should be deployed within the straight segment of the precavernous portion of the distal extracranial internal carotid artery. Balloon predilatation can be performed using a 4.0 mm balloon catheter. If an EPD cannot cross a lesion initially, a 0.014-inch floppy guidewire can be used, and the lesion can be inflated with a small (2.0 mm) coronary balloon catheter before a repeat attempt to advance the EPD across the lesion. Atropine 0.5 to 1.0 mg is administered prophylactically to minimize the incidence of transient severe bradycardia during stretching of the carotid body if the resting heart rate is <60 beats/min. Using the guidance of bony landmarks or an angiographic roadmap, a self-expanding stent then is positioned and carefully deployed across the lesion. Postdilatation using a balloon catheter that matches the reference diameter of the internal carotid artery then is performed. For a carotid bifurcation lesion, the diameter of the self-expanding stent should match the diameter of the common carotid artery, and the length of the stent should be chosen to fully cover the lesion. The EPD then is retrieved, and angiography is performed for the target lesion as well as the intracerebral arteries supplied by the vessel in order to detect any distal embolization. When slow flow is noted on the angiogram before filter retrieval, this usually represents the filter being overwhelmed by the embolized material, or fibrin; a 125 cm-long diagnostic catheter or an aspiration catheter can be advanced over the EPD to aspirate the stagnant blood column before retrieving the filter. Access closure is usually recommended. The operator should then perform a brief neurologic examination before transferring the patient to the recovery area.
symptoms despite appropriate medical therapy. The procedure is high-risk and technically challenging, and it requires a fund of knowledge of the intracranial arterial anatomy and physiology, and a high level of technical expertise. A multidisciplinary team consisting of a clinical neurologist, a neuroradiologist, and an interventionalist who is familiar with small vessel angioplasty and stenting is recommended to provide optimal care and clinical outcomes. To provide primary endovascular therapy for acute stroke, we adopt a model similar to acute MI treatment in the Ochsner Clinic, with both the on-call neurologist and interventionalist available round-the-clock to make appropriate patient selection and treatment.
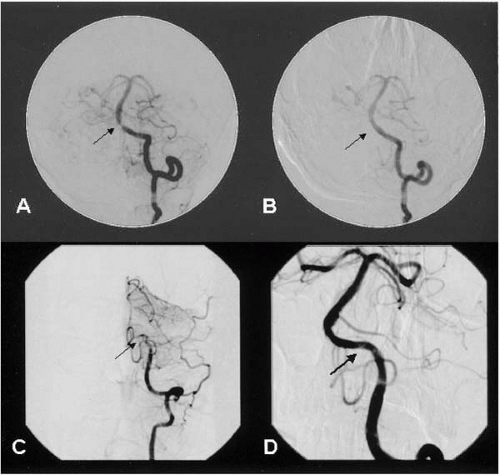 Figure 20.5. (A) A 52-year-old man had symptom of vertebrobasilar insufficiency associated with a severe focal stenosis at the junction of the vertebral and basilar arteries (arrow). (B) The stenosis was relieved after revascularization with a balloon-expandable stent (arrow). (C) Two years later, he presented with intermittent headache, diplopia, and nausea. Selective angiography revealed occlusion in the V4 segment (arrow). (D) The occlusion was recanalized with a Choice PT extra-support guidewire, and satisfactory angiographic result was achieved after stent placement (Express 3.5 × 12 mm, 3.0 × 12 mm, and two 3.0 × 8 mm stents) (arrow). |
selectively engage the ostium of the target vessel. Guide catheter manipulation should be kept at a minimum because of the atheromatous disease burden in the aorta commonly found in patients with renal atherosclerosis. A 4 to 5 Fr diagnostic catheter (IMA, Bernstein, SOS, Simmons, or Cobra) may be useful to assist the selective engagement of the guide catheter. A soft-tipped 0.014-inch steerable coronary guidewire and an undersized balloon may be used for predilatation when stent placement is intended. A 1:1 balloon-to-artery ratio should be used to treat fibromuscular dysplasia. Patients should be monitored for the presence of back pain during balloon inflation, because it may signify overstretching of the adventitia and that the use of a larger balloon should be avoided.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


