Peripheral arterial disease (PAD) describes the pathologic states that lead to stenoses and aneurysms in the noncoronary arterial circulation. This chapter focuses on the diseases of the arterial supply to the extremities and the renal vasculature (disease states involving the aorta and cerebral vasculature are discussed elsewhere in this volume). PAD can be classified as occlusive or aneurysmal. Atherosclerosis is the most common cause of PAD. In aneurysmal states, weakening of the arterial media results in focal dilatation of the artery to at least 1.5 times the normal diameter. These aneurysmal segments can subsequently dissect, rupture, or thrombose, with catastrophic consequences. In addition to atherosclerosis, there are several less common pathologies that can cause PAD, including vasculitis, arterial injury, entrapment syndromes, and cystic adventitial disease. These disorders are beyond the scope of this chapter.
II. LOWER EXTREMITY PERIPHERAL ARTERY DISEASE
A. Etiology and natural history.
Atherosclerosis is the most common cause of lower extremity PAD. Traditional risk factors include age, smoking history, diabetes mellitus, hyperlipidemia, and hypertension. Emerging risk factors include elevated markers of inflammation such as C-reactive protein, fibrinogen, and interleukin 6; chronic kidney disease; hypercoagulable states such as hyperhomocysteinemia; and possibly a genetic predisposition to PAD. African Americans have a twofold increase in risk of developing PAD. The prevalence of PAD increases significantly with age, such that the prevalence is 2% to 3% in persons aged ≤ 50 years and up to 20% in persons aged > 70 years. Fibromuscular dysplasia (FMD), a noninflammatory and nonatherosclerotic process, can also affect the lower extremities by causing hyperplastic cell growth and luminal narrowing, although it predominantly affects the renal and carotid arteries. Patients with lower extremity PAD may present with leg symptoms or may be entirely asymptomatic. Approximately 50% of patients > 55 years old with PAD, with or without claudication symptoms, when followed for 5 years will remain stable or improve with exercise and lifestyle modifications. The remaining 50% will have progressive worsening of symptoms, and approximately 4% will require major amputation if they do not undergo revascularization. The highest risk of amputation occurs in those patients who are diabetic and continue to smoke. Cardiac disease accounts for the majority of deaths in patients with PAD, in whom the relative risk of death from cardiac causes is increased more than sixfold. Approximately one-third to one-half of all patients with PAD will have concomitant coronary disease depending on the diagnostic criteria utilized, and thus PAD is considered a coronary artery disease risk equivalent.
B. Clinical manifestations
1. Signs and symptoms.
Rest perfusion of the lower extremities may be adequate; however, if the arterial stenosis is severe, then exercise may precipitate ischemia and claudication. Symptoms may include pain, discomfort, or fatigue of the buttock, thigh, or calf musculature and are usually gradual in onset. The amount of exercise required to precipitate pain is roughly related to the severity of the stenosis. Pain is usually manifested one segment below the area of severe stenosis (Table 27.1), and the most frequently involved artery in intermittent claudication is the superficial femoral artery. The symptoms are usually promptly relieved with rest or standing. More severe stenosis or more distal atherosclerotic lesions may result in limb-threatening ischemia with foot pain at rest, tissue ulceration, or gangrene. There are two terms frequently used to describe this condition that should be differentiated: critical limb ischemia and acute limb ischemia. Critical limb ischemia is resting limb pain that results from severe atherosclerotic disease that compromises distal blood flow of the involved limb. This term is typically used to describe chronic lesions such as ischemic rest pain, ischemic ulcers, or gangrene and is caused by a slow progression of atherosclerotic disease. Acute limb ischemia occurs abruptly and threatens the viability of the involved tissue. Acute limb ischemia is usually the result of an embolic event or arterial thrombosis.
2. Physical examination.
Characterization of femoral, popliteal, dorsalis pedis, and posterior tibial pulses; auscultation for bruits in the abdomen and bilateral groins; and palpation for aneurysm in the abdomen and over the popliteal arteries are all part of a comprehensive lower extremity vascular examination. A complete cardiac examination and auscultation of carotid arteries should also be performed to assess for concurrent abnormalities, given the common atherosclerotic pathogenesis of cerebral, myocardial, and peripheral arterial disease. Signs of lower extremity arterial insufficiency can include coolness, dry skin and scaling, pallor that is worsened with leg elevation, and ulcerations. Rarely muscular atrophy can be seen. The evaluation of a patient with possible acute limb ischemia should include the “5 P’s”: pain, pallor, pulselessness, paresthesias, and paralysis. These clinical features have prognostic value in acute limb ischemia (Table 27.2).
TABLE 27.1 Localization of Peripheral Arterial Disease
The ABI is a measurement of lower extremity perfusion, which compares the blood pressure in a pedal artery with the higher of two brachial artery blood pressures. The ABI cannot localize stenosis, but is a simple and accurate measure of disease severity (Table 27.3). In general, ABI value correlates poorly with symptoms, and two patients with the same ABI may have remarkably different complaints. Symptoms at rest rarely occur, unless the ABI is < 0.4 (i.e., critical limb ischemia). The ABI has limited use in noncompressible, calcified vessels. In patients with noncompressible ankle vessels (ABI > 1.4) the toe—brachial index can be used in conjunction with pulsevolume recordings (PVRs) to document PAD. Measuring the ABIs before and after exercise can help diagnose PAD when the resting ABI is normal but there is a high clinical suspicion for PAD. It can also help differentiate between true claudication and nonarterial leg pain (pseudoclaudication).
2. Pulse-volume recordings.
PVRs detect changes in the volume (arterial flow) of the limb during the cardiac cycle. Blood pressure cuffs are placed at the thigh (one or two cuffs), calf, ankle, midfoot, and toe. The change in volume of the respective cuff during the cardiac cycle identifies the presence of arterial stenosis by reduction in the pulsatile flow as detected by changes in pulse contour and amplitude at that cuff, as documented by the PVR waveform (Fig. 27.2). Segmental blood pressure measurements may be taken along the leg with the segmental PVR tracings for localization of disease. Unlike ABIs, arterial calcification does not effect PVR tracings, and PVR can often be helpful in the diabetic patient with a foot ulcer and suspected arterial calcification.
TABLE 27.2 Categorizing Acute Limb Ischemia
Category
Prognosis
Sensory loss
Muscle weakness
Arterial Doppler signal
Venous Doppler signal
Viable
Not immediately threatened
None
None
Audible
Audible
Threatened marginally
Salvageable if promptly treated
Minimal (toes) or none
None
Often inaudible
Audible
Threatened immediately
Salvageable with immediate revascularization
More than toes, rest pain
Mild, moderate
Usually inaudible
Audible
Irreversible
Major tissue loss or permanent nerve damage
Profound anesthesia
Profound paralysis
Inaudible
Inaudible
Adapted from Katzen BT. Clinical diagnosis and prognosis of acute limb ischemia. Rev Cardiovasc Med. 2002;3(suppl 2):S2-S6.
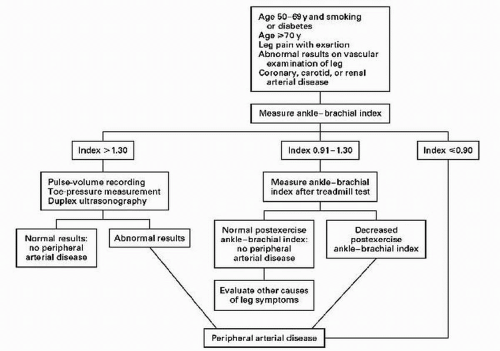
FIGURE 27.1 Evaluation of patients in whom peripheral arterial disease is suspected. (Reproduced from Hiaat WR. Medical treatment of peripheral arterial disease and claudication. N Engl J Med. 2001;344:1608, with permission.)
3. Duplex ultrasound.
Arterial duplex renders an anatomic assessment of the arterial system using a combination of B-mode ultrasound imaging and Doppler frequency spectral analysis. Doppler complements the standard qualitative ultrasound imaging by allowing waveform analysis and assessment of Doppler velocities. Using the concept that velocity of blood flow increases as it flows through a stenotic lesion, peak systolic and end-diastolic velocities are measured and used to estimate the severity of a stenosis. This modality is useful for anatomic visualization of lesions and for surveillance after stenting or bypass grafting.
TABLE 27.3 Evaluating Disease Severity with the Ankle-Brachial Index
ABI
Interpretation
1.3
Noncompressible vessel
1.0-1.29
Normal
0.91-0.99
Equivocal
0.4-0.90
Mild to moderate PAD
<0.4
Severe PAD
ABI, anklebrachial index.
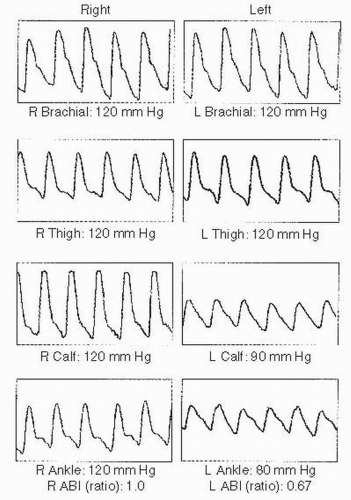
FIGURE 27.2 Pulse-volume recording (PVR) of the lower extremities. This PVR was obtained from a 42-year-old man with a history of diabetes mellitus and tobacco use who developed new left calf cramping with exertion. It demonstrates moderate disease (ankle-brachial index [ABI] = 0.66) of left femoropopliteal segment and a normal recording on the right lower extremity. He was advised to begin both a tobacco cessation program and a walking regimen.
4. Magnetic resonance angiography (MRA).
Only gold members can continue reading. Log In or Register to continue