Chapter 55
Peripheral Arterial Disease
1. What are the key components of the vascular physical examination?
 Blood pressure measurements in both arms
Blood pressure measurements in both arms
 Carotid pulse palpation for upstroke and amplitude, and auscultation for bruits
Carotid pulse palpation for upstroke and amplitude, and auscultation for bruits
 Auscultation of the abdomen and flank for bruits
Auscultation of the abdomen and flank for bruits
 Palpation of the abdomen for aortic pulsation and its maximal diameter
Palpation of the abdomen for aortic pulsation and its maximal diameter

 Performance of the Allen test when knowledge of hand perfusion is needed
Performance of the Allen test when knowledge of hand perfusion is needed
 Auscultation of the femoral arteries for the presence of bruits
Auscultation of the femoral arteries for the presence of bruits
 Inspection of the feet for color, temperature, and integrity of the skin, and for ulcers
Inspection of the feet for color, temperature, and integrity of the skin, and for ulcers

2. Can the location of the patient’s lower extremity claudication help to localize the site of occlusive disease?
 Occlusive iliac artery disease may produce hip, buttock, and thigh pain, as well as calf pain.
Occlusive iliac artery disease may produce hip, buttock, and thigh pain, as well as calf pain.
 Occlusive femoral and popliteal artery disease usually produces calf pain.
Occlusive femoral and popliteal artery disease usually produces calf pain.

3. What noninvasive tests are used in the assessment of lower limb claudication?
 Ankle-brachial index (ABI): The ankle-brachial index is the ankle systolic pressure (as determined by Doppler) divided by the brachial systolic pressure. An abnormal index is less than 0.90. The sensitivity is approximately 90% for diagnosis of PAD. (See Question 4 for further details.)
Ankle-brachial index (ABI): The ankle-brachial index is the ankle systolic pressure (as determined by Doppler) divided by the brachial systolic pressure. An abnormal index is less than 0.90. The sensitivity is approximately 90% for diagnosis of PAD. (See Question 4 for further details.)



 Exercise testing: This testing determines treadmill walking time and preexercise and postexercise ABI. In those without significant PAD, the ABI is unchanged after exercise. In patients with PAD, the ABI falls after exercise. This test is more sensitive for detecting disease than a resting ABI alone.
Exercise testing: This testing determines treadmill walking time and preexercise and postexercise ABI. In those without significant PAD, the ABI is unchanged after exercise. In patients with PAD, the ABI falls after exercise. This test is more sensitive for detecting disease than a resting ABI alone.
Experts emphasize that the ABI is a continuous variable below 0.90. Values of 0.41 to 0.90 are considered to be mildly to moderately diminished; values of 0.40 or less are considered to be severely decreased. An ABI of 0.40 or less is associated with an increased risk of rest pain, ischemic ulceration, or gangrene. Patients with long-standing diabetes or end-stage renal disease on dialysis and elderly patients may have noncompressible leg arterial segments caused by medial calcification, precluding assessment of the ABI. These patients are best evaluated using digital pressures and with assessment of the quality of the arterial waveform in the PVR studies. A system for interpretation of the ABI is given in Table 55-1.
TABLE 55-1
INTERPRETATION OF THE ANKLE-BRACHIAL INDEX
| ABI | Interpretation |
| >1.30 | Noncompressible |
| 1.00-1.29 | Normal |
| 0.91-0.99 | Borderline (equivocal) |
| 0.41-0.90 | Mild to moderate PAD |
| 0.00-0.40 | Severe PAD |
ABI, Ankle-brachial index; PAD, peripheral arterial disease.
Modified from Hiatt WR: Medical treatment of peripheral arterial disease and claudication, N Engl J Med 344:1608-1621, 2001.
5. What are the recommended medical therapies and lifestyle interventions in patients with lower extremity PAD?
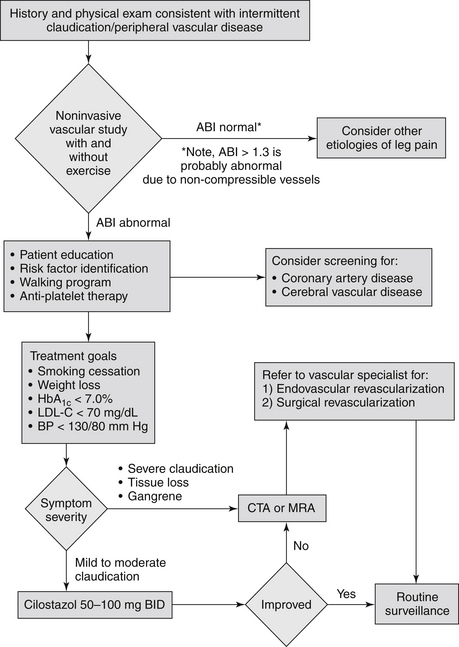
A supervised exercise regimen is recommended as the initial treatment modality for patients with intermittent claudication. Supervised exercise training is recommended over unsupervised exercise training. Cilostazol treatment can lead to a modest increase in exercise capacity. Because agents with similar biologic effects have been shown to increase mortality in patients with heart failure, this drug should not be used in patients with heart failure. Smoking cessation must be strongly emphasized to the patient. Other measures include general secondary prevention interventions. Recommended medical therapies and lifestyle interventions in patients with lower extremity PAD are summarized in Box 55-1. An algorithm for the management of patients with suspected peripheral arterial disease is presented in Figure 55-1.
Box 55-1 RECOMMENDED MEDICAL THERAPIES AND LIFESTYLE INTERVENTIONS IN PATIENTS WITH LOWER EXTREMITY PERIPHERAL ARTERIAL DISEASE
 Statin treatment to lower LDL level to <70-100 mg/dL
Statin treatment to lower LDL level to <70-100 mg/dL



 Patients with PAD should be offered smoking cessation interventions.
Patients with PAD should be offered smoking cessation interventions.
 Antiplatelet therapy is indicated to reduce the risk of MI, stroke, or vascular death.
Antiplatelet therapy is indicated to reduce the risk of MI, stroke, or vascular death.





Modified from Hirsch AT, Haskal ZJ, Hertzer NR, et al: ACC/AHA guidelines for the management of patients with peripheral arterial disease, J Am Coll Cardiol 47(6):1239-1312, 2006.