The Seattle Heart Failure Model (SHFM) is a validated multivariate risk prediction model for mortality in patients with heart failure, using widely available clinical variables. The aim of this study was to assess the performance of the SHFM when applied to patients with heart failure who received cardiac resynchronization therapy devices with defibrillation. A total of 413 patients were identified from 2 prospective implantable cardioverter-defibrillator registries who received cardiac resynchronization therapy devices with defibrillation for the primary prevention of sudden death. Baseline laboratory and clinical data were entered in the SHFM to calculate predicted survival. The end point was all-cause mortality. During a median follow-up period of 2.8 years, 78 patients died and 9 underwent heart transplantation. Observed versus predicted 5-year mortality rates were 11.6% versus 11.4%, 21.5% versus 22.1%, and 41.4% versus 46.1% by ascending tertile of Seattle Heart Failure Score, respectively. No systematic or substantial errors of risk estimation were observed. Discrimination was excellent; the C-statistic ranged from 0.78 at 1-year follow-up to 0.70 at 5-year follow-up, and the Hosmer-Lemeshow chi-square statistic was 0.87 (p = 0.65). In conclusion, in patients with heart failure who received cardiac resynchronization therapy devices with defibrillation, the SHFM offers adequate discrimination of risk for all-cause mortality and estimation of mortality risk without substantial or systematic errors.
Appropriate risk prediction in patients with heart failure (HF) is of high importance, to decide whether the potential benefits of an intervention additional to medical therapy for a certain patient outweigh its risks and to be able to inform the patient about prognosis. The Seattle Heart Failure Model (SHFM) is a validated multivariate risk prediction model for mortality in patients with HF. The utility of this model was recently evaluated in patients enrolled in the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Because not all required SHFM covariates were registered in SCD-HeFT, a modified version of the SHFM (i.e., SHFM-D, including differential implantable cardioverter-defibrillator [ICD] benefit) was developed. The performance of the SHFM-D was excellent in predicting survival in primary prevention ICD patients. However, the performance of the SHFM-D in patients with HF who received ICDs combined with cardiac resynchronization therapy (CRT-D) is unknown. The purpose of this study was to assess the predictive value (i.e., calibration and discrimination) of the SHFM when applied to a real-world cohort of primary prevention CRT-D patients.
Methods
We used data from prospective ICD registries of the cardiology departments of Erasmus MC (Rotterdam, The Netherlands) and the University Hospital of Basel (Basel, Switzerland). We identified all patients who received first implantations of CRT-D devices for the primary prevention of sudden cardiac death from January 2000 and October 2009. The following selection criteria for cardiac resynchronization therapy were applied: symptomatic HF despite optimal drug therapy, an impaired left ventricular ejection fraction (≤35%), and the presence of an inter- or intraventricular conduction delay (QRS duration ≥120 ms). Primary prevention as an indication for ICD therapy was defined as the presence of a left ventricular ejection fraction ≤35% with ischemic or nonischemic cardiomyopathy without a history of cardiac arrest or sustained ventricular arrhythmia. The administrative censoring date was the end of October 2010 for all patients alive until that date.
Demographic and clinical data were obtained before CRT-D implantation. If multiple laboratory data were available, values from the date closest to the date of implantation were used; all laboratory values obtained up to 7 days before CRT-D implantation were accepted.
The SHFM is a validated risk prediction model that uses widely available clinical variables to predict prognosis and the impact of therapy on survival. The original SHFM was derived from the Prospective Randomized Amlodipine Survival Evaluation (PRAISE I) database and prospectively validated in 3 populations from clinical trials and in 2 outpatient practice settings. The recent SHFM-D model included the original SHFM variables age, gender, weight, systolic blood pressure, New York Heart Association class, the left ventricular ejection fraction, cause of left ventricular dysfunction, medication use (angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, β-blockers, and statins), daily diuretic dose (furosemide, bumetanide, torsemide, metolazone, and hydrochlorothiazide), and the laboratory values of serum sodium, as well as the new variables of digoxin use, carvedilol use, and serum creatinine. Because hemoglobin, a variable in the original SHFM, was available in all patients, this variable was also added to the SHFM-D using the original data set (10,038 patients) to derive the β coefficient. The effectiveness of CRT-D in reducing mortality was estimated using a fixed hazard ratio of 0.64 across the SHFM-D risk spectrum, as in the original SHFM (W.C. Levy, personal communication). For simplicity, we use the term “SHFM” instead of “SHFM-D” throughout this report.
Follow-up started at the time of CRT-D implantation. In Rotterdam, patients were seen at 10 days; at 3, 6, 9, and 12 months after implantation; and at 6-month intervals thereafter. In Basel, patients were seen at 1, 3, and 6 months after implantation and also at 6-month intervals thereafter. The follow-up visits included clinical assessment and device interrogation. The end point for this study was all-cause mortality; patients who underwent heart transplantation were censored alive on the day of transplantation. Deaths were classified according to a modified Hinkle-Thaler system.
Continuous variables are presented as mean ± SD if normally distributed or otherwise as medians and interquartile ranges (IQRs). Data were compared using Student’s t test or the Mann-Whitney U test as appropriate. Categorical data are expressed as percentages and were compared using Fisher’s exact test. For all patients, the Seattle Heart Failure Score (SHFS) was calculated as previously described by Levy et al. In case of missing data, the covariate was imputed with the cohort mean of the respective continuous variables. Subsequently, the SHFS was converted to event-free survival probabilities up to 5 years for each individual patient (i.e., predicted survival). The observed survival rates were calculated according to the Kaplan-Meier method, and differences were evaluated using the log-rank test. Calibration of SHFM was assessed by (1) the SHFM-predicted survival plotted against observed survival at 1 and 5 years and (2) the Hosmer-Lemeshow goodness-of-fit test. Discrimination was assessed by (1) the C-statistic for time-to-event data and (2) the 1- and 5-year area under the receiver-operating characteristic curve (AUC). The AUC and C-statistic can range from 0.5 (no discrimination) to 1.0 (perfect discrimination).
Cox proportional-hazards models were used to analyze the relations between SHFS and mortality. The proportional-hazards assumption was tested by assessing log-log survival curves and using Schoenfeld residuals. Hazard ratios are presented with corresponding 95% confidence intervals (CIs). Statistical analysis was performed using Stata version 11 SE for Windows (StataCorp LP, College Station, Texas) and PASW version 18 (IBM Corporation, Somers, New York). Statistical significance was defined as p <0.05 (2 tailed).
Results
The study cohort consisted of 413 patients with HF who underwent first implantation of CRT-D devices for the primary prevention of sudden cardiac death (299 [72%] from Rotterdam and 114 [28%] from Basel). The baseline characteristics of the study population are presented in Table 1 .
| Variable | Total (n = 413) | Tertile 1 (n = 137) | Tertile 2 (n = 138) | Tertile 3 (n = 138) | p Value |
|---|---|---|---|---|---|
| Demographics | |||||
| Age (years) | 61 ± 12 | 55 ± 13 | 63 ± 9 | 66 ± 9 | <0.001 |
| Men | 314 (76%) | 101 (74%) | 101 (73%) | 112 (81%) | 0.32 |
| Weight (kg) | 81 ± 16 | 83 ± 18 | 82 ± 15 | 79 ± 14 | 0.05 |
| HF characteristics | |||||
| NYHA class II | 139 (34%) | 82 (40%) | 38 (27%) | 19 (13%) | <0.001 |
| NYHA class III | 264 (64%) | 55 (60%) | 95 (69%) | 114 (83%) | <0.001 |
| NYHA class IV | 10 (2%) | 100 (0%) | 5 (7%) | 115 (4%) | <0.001 |
| Ejection fraction (%) | 24 ± 7 | 25 ± 7 | 23 ± 7 | 23 ± 7 | 0.01 |
| QRS duration (ms) | 165 ± 30 | 163 ± 29 | 163 ± 30 | 168 ± 30 | 0.23 |
| Ischemic cause of HF | 194 (47%) | 40 (29%) | 74 (54%) | 80 (58%) | <0.001 |
| Persistent atrial fibrillation | 52 (13%) | 6 (4%) | 25 (18%) | 21 (15%) | <0.001 |
| Systolic blood pressure (mm Hg) | 117 ± 19 | 125 ± 18 | 117 ± 16 | 108 ± 19 | <0.001 |
| Hemoglobin (g/dl) | 13.4 ± 1.8 | 14.1 ± 1.4 | 13.7 ± 1.8 | 12.7 ± 1.9 | <0.001 |
| Serum sodium (mmol/L) | 138 ± 4 | 139 ± 4 | 139 ± 4 | 137 ± 4 | <0.001 |
| Serum BUN (mg/dl) (median) | 24.4 | 19.6 | 23.8 | 33.9 | <0.001 |
| Serum creatinine (mg/dl) (median) | 1.2 | 1.0 | 1.1 | 1.5 | <0.001 |
| Medications | |||||
| ACE inhibitors | 343 (83%) | 115 (83%) | 109 (79%) | 121 (88%) | 0.15 |
| Angiotensin receptor blockers | 104 (25%) | 37 (27%) | 38 (28%) | 29 (21%) | 0.38 |
| β blockers | 324 (79%) | 125 (91%) | 110 (80%) | 89 (65%) | <0.001 |
| Carvedilol | 136 (33%) | 53 (38%) | 51 (36%) | 32 (24%) | 0.02 |
| Digoxin | 112 (27%) | 17 (12%) | 34 (25%) | 61 (44%) | <0.001 |
| Diuretics | 357 (86%) | 198 (72%) | 127 (92%) | 132 (96%) | <0.001 |
| Spironolactone | 189 (46%) | 48 (35%) | 75 (54%) | 66 (48%) | 0.005 |
| Allopurinol | 41 (10%) | 7 (5%) | 10 (7%) | 24 (17%) | 0.001 |
| Statins | 232 (56%) | 78 (57%) | 82 (59%) | 72 (52%) | 0.47 |
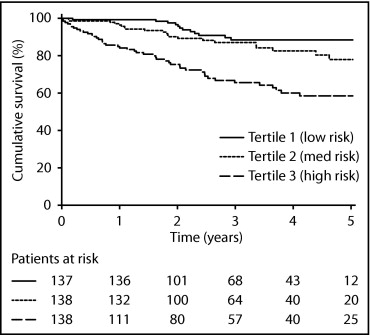
During a median follow-up period of 2.8 years (IQR 1.7 to 4.6), 78 patients (19%) died and 9 patients (2%) underwent heart transplantation. Of the 78 deaths, 61 (78%) were classified as cardiac (9 sudden and 52 nonsudden) and 9 (12%) as noncardiac. The causes of death were unknown in 8 cases. The median interval from device implantation to death was 1.7 years (IQR 0.7 to 2.4). The observed cumulative incidence of mortality was 6.6%, 13.1%, and 25.3% at 1, 2, and 5 years, respectively. The median SHFS was higher for patients who died compared to those who survived (0.66 [IQR 0.04 to 1.06] vs −0.06 [IQR −0.51 to 0.47], p <0.001). Subsequently, the study population was stratified by ascending risk tertiles of SHFS (i.e., low to high risk). The baseline characteristics according to SHFS tertiles are listed in Table 1 . Total mortality by ascending risk tertile of SHFS was 8.8% (n = 12), 14.5% (n = 20), and 33.3% (n = 46) (p <0.001). The observed cumulative incidence of mortality stratified by SHFS tertiles is shown in Figure 1 .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


