Classa
Levelb
Surgery is indicated in symptomatic pts with severe TSc
I
c
Surgery is indicated in pts with severe TS undergoing left-sided valve surgeryd
I
c
Surgery is indicated in pts with severe primary or secondary TR undergoing left-sided surgery
I
c
Surgery should be considered in pts with moderate primary TR undergoing left-sided valve surgery
IIa
c
Surgery should be considered in pts with mild or moderate secondary TR with dilated annulus (≥40 mm or >21 mm/m2) undergoing left-sided valve surgery
IIa
c
Surgery should be considered in asymptomatic or mildly symptomatic pts with severe isolated primary TR and progressive RV dilatation or deterioration of RV function
IIa
c
After left-sided valve surgery, surgery should be considered in pts with severe TR who are symptomatic or have progressive RV dilatation dysfunction, in the absence of left-sided valve dysfunction and severe pulmonary vascular disease
IIa
c
37.3 Technique of PTVI
Patients are treated using conscious sedation or general anesthesia. If not performed before, a transesophageal echocardiogram is done for assessment of valve regurgitation and the inflow gradient across the tricuspid valve. Then vascular access (vein and artery) is achieved usually in the groin. Valve delivery via a venous neck vessel has been described as well. Pressures at right atrial and right ventricular level are recorded. The difference between the A wave in the right atrium and the right ventricular end-diastolic pressure in mmHg is assessed (TrV-inflow gradient). Most bioprostheses in the TrV position are mounted in a non-distensible ring offering a safe landing zone for a percutaneous valve. Using fluoroscopy the metallic cage of the bioprosthesis is usually visible and is an excellent landmark during valve implantation. An aortogram depicts the course of the right coronary artery in relation to the bioprosthesis. A “balloon interrogation,” however, is rarely necessary since the metallic frame of the bioprosthesis prevents coronary compression. An angiogram within the right ventricle is performed (RV function and degree of tricuspid regurgitation) (Fig. 37.1). Accurate valve placement requires coaxial positioning within the bioprosthesis. The x-ray system is rotated to a complete perpendicular position in the anterior posterior plane which is used for valve delivery. A 0.0035 in. superstiff guidewire is placed distally into one pulmonary artery. This position adds additional safety during valve delivery since a guidewire position in the right ventricle is less stable. Even if the type of bioprosthesis in tricuspid position is known, a balloon test is performed to determine the actual inner diameter of the prosthesis (Fig. 37.2). The balloon chosen for this test should be at least 2 mm larger than the suspected internal bioprosthesis valve diameter. Valuable information on current biological valves and their dimensions are available in the literature [2]. In our practice, a Melody valve is chosen if the internal diameter is <24 mm (Fig. 37.3). In larger internal valve diameters, the Edwards Sapien 26 mm or Sapien 29 mm may be used. If the internal diameter of the bioprosthesis is at least 2 mm less than the external diameter of the inflated implanted valve, pre-stenting is not necessary. In large valves, the internal diameter may be reduced by pre-stenting with CP stents. Dilation of a covered 8 zig CP stent to a large diameter leads to significant shortening of the stent. For this reason in our practice, at least a 39 mm or preferably a 45 mm long covered CP stent should be used. If this stent is mounted on a large balloon, a large long sheath for stent delivery is necessary. The groin needs to be dilated prior to valve implantation. For the Melody valve a short 22 F dilator is used since the delivery catheter is 22 F. The valve is mounted in the same way as it is described for percutaneous pulmonary valve implantation. Edwards supplies excellent hydrophilic dilators for pre-dilation of the groin. In contrast to the retrograde positioning in the aortic valve, the Sapien 26 and 29 valves need to be pre-mounted the other way around (180° opposite than in aortic valve delivery) to account for the antegrade positioning. The Sapien 26 valve is mounted on the Retroflex 3 catheter system which is introduced through a 24 F hydrophilic sheath into the inferior vena cava. The Sapien XT 29 valve is mounted on the shaft of the NovaFlex + transfemoral system which is introduced via the eSheath (20 F) into the patient. Within the patient this valve is then pulled onto the delivery balloon against the direction of the valve leaflets. Although this described procedure is “off label” and there is some concern relating to damage of the valve leaflets when pulling them against the direction of blood flow, in our experience all those implanted Sapien XT valves show excellent function during short- and medium-term follow-up.
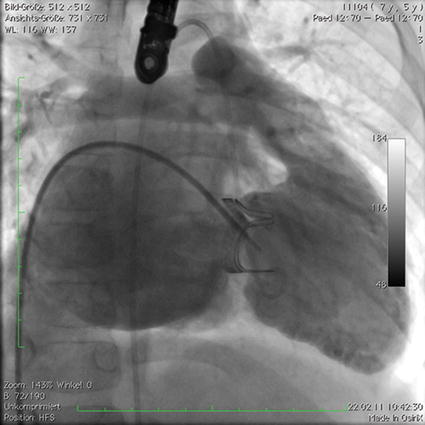
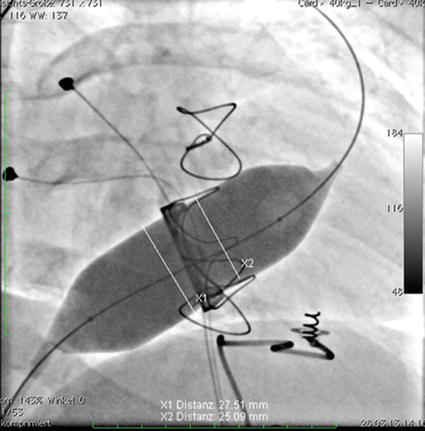




Fig. 37.1
Injection of contrast into the right ventricle of a patient with Ebstein’s anomaly after implantation of a Carpentier-Edwards Perimount 27 mm bioprosthesis (Edwards Lifesciences, Irvine, CA). Severe tricuspid regurgitation stains the enlarged right atrium
Fig. 37.2
A balloon interrogation test is performed with a 28 mm diameter Z-MED II-XTM balloon (NuMed Inc. Best, The Netherlands) in a patient with Ebstein’s anomaly after three operations. Finally a Carpentier-Edwards Perimount 31 mm bioprosthesis had been implanted. The minimal diameter was 25 mm
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
