Fig. 20.1
Right venous femoral access, ilio-caval catheterization followed by left renal vein catheterization: venous drainage of a large left gonadal vein (a), in a context of chronic pelvic venous congestion, documented in this 48 y. o. W by noninvasive imaging (CT + Doppler) and confirmed by these selective catheterizations and injection in the lower left ovarian vein (b)
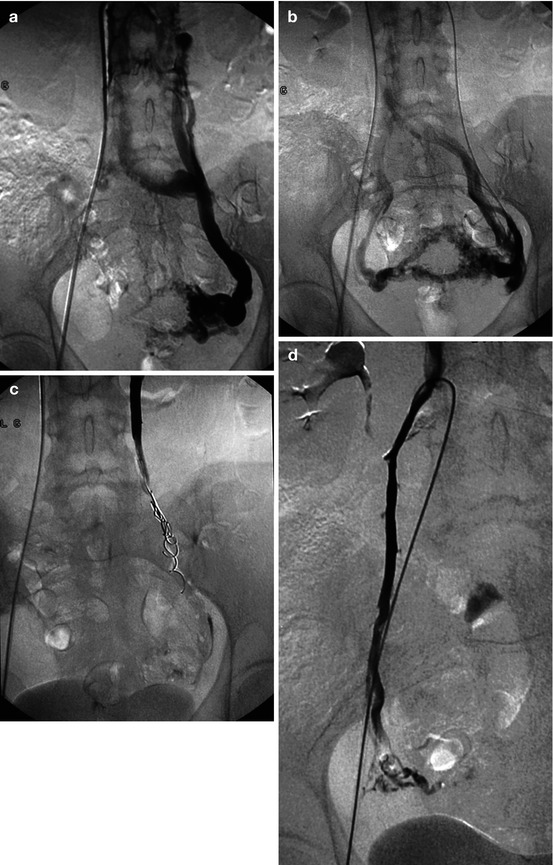
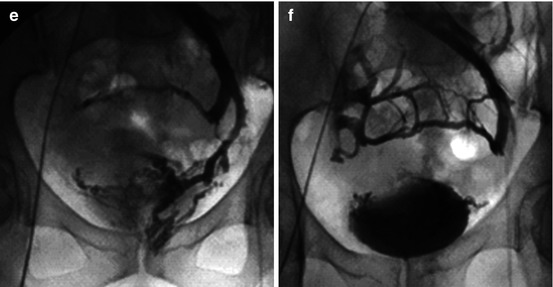
Fig. 20.2
A 45 y. o. W, clinical + radiological suspicion of chronic pelvic venous congestion syndrome. (a, b) Selective injection after catheterization of the left gonadal vein: pelvic venous congestion, opacification of the right gonadal vein (b) via the pelvic anastomosis. (c) Control after left ovarian vein embolization with tetradecyl sulfate + coils. (d) Right gonadal vein catheterization: coils + sclerosing agent embolization. (e, f) Additional pelvic embolization 4 weeks later: left hypogastric vein catheterization from a right venous femoral access (crossover) (e), followed by embolization beyond an occlusion balloon (f)
References
1.
Belenky A, Bartal G, Atar E, Cohen M, Bachar GN. Ovarian varices in healthy female kidney donors: incidence, morbidity, and clinical outcome. Am J Roentgenol. 2002;179:625–9.CrossRef
2.
3.
Beard RW, Highman JH, Pearce S, Reginald PW. Diagnosis of pelvic varicosities in women with chronic pelvic pain. J Obstet Gynaecol. 1988;95:153–61.CrossRef
4.
Beard RW, Highman JH, Pearce S, et al. Diagnosis of pelvic varicosities in women with chronic pelvic pain. Lancet. 1984;2:946–9.PubMedCrossRef
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


