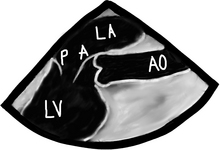
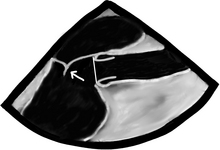
Chapter 11 Pathology of the Cardiac Valves F. Luke Aldo and Enrique Pantin Cardiac valves… hopefully somewhere somebody talked about normal valves… Normal systolic blood velocities through the valves are: Valves and their supporting structures can sustain several types of damage that can cause them to malfunction. For simplicity, valve dysfunction has been categorized as stenosis or insufficiency. Before we continue any further we must always make sure in cases of valvular stenosis that the problem is at the valve level and not a sub- or supra-valvular stenosis. It takes years to develop tight valves, and thus it takes a while to cause problems. Leaky valves can occur over years, but also acutely. As you can imagine, acute valve leakage is not well tolerated by the heart. This often needs immediate medical intervention and usually surgical repair as the heart has no time to compensate for the extra volume load. We are going to concentrate on the two valves that most commonly develop problems, the aortic and the mitral. When assessing valves we use 2-D imaging and Doppler-related measurements: continuous wave Doppler (for faster velocities, usually greater than 2–2.5 m/s), pulsed-wave Doppler (for slower velocities, anything less than 2–2.5 m/s), and color flow Doppler (will give us an idea about what the blood flow pattern is). We can also use 3-D, but this is a bit esoteric for us. We know what the normal velocities through the valves are and that if the valve gets narrower, in order to allow the passage of the same stroke volume the blood velocity through the smaller orifice will increase proportionally. This is valve stenosis in action. That is it, you’ve got it! End of chapter, we can stop writing! You wish! Valvular regurgitation is diagnosed when we see diastolic valvular flow in the opposite direction it should be going. Now we are really done! Just kidding, we will explore stenosis and regurgitation a bit more. In a tube with an area of focal stenosis: There are a bunch of images and numbers used to categorize the degree of valvular dysfunction. You should always look at the supra-valvular, valvular, and infra-valvular areas. For the aortic valve the mid esophageal long and short axis, and then the deep transgastric views are ideal. The first two will provide a lot of anatomical data and the last one is the best for Doppler measurements. In the ME AV LAX view (during systole and diastole) the areas above, below, and at the level of the valve can be examined in 2-D and then color flow Doppler. The first image below is named Mid Esophageal Aortic Valve LAX (Long Axis) view and is usually obtained at a multiplane angle of about 130 degrees. The image was taken in ventricular diastole; note that the mitral valve is open, and the aortic valve is closed. LA = left atrium; P = posterior mitral valve leaflet; A = anterior mitral valve leaflet (the anterior mitral leaflet is always the closest to the aortic valve); LV = left ventricle; AO = ascending aorta. The anterior mitral leaflet in this image corresponds to a segment of the mitral leaflet called “A2”. “A2” length measurement correlates very closely with the ideal mitral valve ring size that needs to be used when a surgeon performs a mitral valve repair in cases of mitral regurgitation. Hey, you can teach this to your surgeon! The second image is in ventricular systole. Notice the closed mitral valve and the amount of mitral leaflet coaptation (arrow), usually greater than 8 mm. A measurement of the aortic valve annulus is taken during systole (white line). This is the best view to measure the aortic annulus. (a) enjoy watching your surgeon stomp his feet like a 2-year-old child who can’t get their way (b) like to see him launch a scalpel across the room like he’s playing a competitive game of darts (c) want to hear him curse like a truck driver (d) want to make him realize he is not the omnipotent deity he thought he once was The following TEE web page is an AMAZING teaching tool, go there and study it: http://pie.med.utoronto.ca/tee/TEE_content/TEE_standardViews_intro.html
NORMAL VALVE AREA
CM2
Aortic valve
3–4
Mitral valve
4–5
Pulmonic valve
3.5–4.5
Tricuspid valve
5–8
Aortic valve
<1.4 m/s
Mitral valve
<1.2 m/s
Pulmonic valve
<1 m/s
Tricuspid valve
<0.8 m/s






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


