FETAL ECHOCARDIOGRAPHY – INDICATIONS AND TECHNIQUE
Introduction
Congenital heart defect (CHD) is the most common abnormal finding in the fetus, with an incidence of 8 to 9 per 1000 live births.1,2 While nearly half of the CHD cases are simple cases that can be corrected with surgery, the rest are significant defects that account for more than half of the deaths from congenital disease in childhood.1 Thus, prenatal diagnosis of CHD is a very important subject for the obstetrician, neonatal specialists, and pediatric cardiologists for optimal care to be given to the mother, fetus, and the newborn baby. With advances in ultrasound imaging, fetal echocardiogram is proved to be a very important diagnostic test to evaluate the structural and functional abnormalities of the fetal heart. In addition to the assessment of the fetal heart, during fetal echocardiography, a very detailed approach should be undertaken to incorporate all the other important factors into the “cardiovascular examination” such as umbilical arterial, venous, and ductus venosus flows and more. Initial cardiac screening is usually done during the obstetric (OB) examination, where at least 4-chamber, left ventricular outflow tract (LVOT) and right ventricular outflow tract (RVOT) views are obtained, as recommended by the International Society of Ultrasound in Obstetrics and Gynecology.3 If cardiac disease is suspected, these cases are referred to pediatric cardiologists specializing in fetal cardiac imaging and diagnosis.
Indications
Even though the majority of CHDs occur in pregnancies without any known risk factors, there are still many identifiable risk factors known to cause cardiac defects. Any of these factors should raise a red flag and have the dyad referred to a center with fetal cardiology expertise. Although the listed factors are the most commonly known, there may be others that may become evident in future as more research is being done on genetic and embryologic causes.4
Fetal Risk Factors
Chromosomal abnormalities, extracardiac defects (eg, omphalocele, diaphragmatic hernia, duodenal atresia, tracheoesophageal fistula, abnormal visceral situs, two-vessel cord, hydrocephalus, microcephalus, hydronephrosis, hydrops), multiple fetal pregnancy, suspicion of twin-to-twin transfusion syndrome (TTTS), and fetal cardiac arrhythmia are among the fetal risk factors.
Maternal Risk Factors
Maternal risk factors include a family or maternal history of CHD, familial or inherited disorders (Marfan’s, Noonan’s, Ellis–van Creveld’s, etc.), diabetes mellitus, autoimmune disease (systemic lupus erythematosus, Sjögren’s), phenylketonuria, decline of invasive prenatal diagnosis in advanced maternal age, abnormal triple screen, and in vitro fertilization.
Exposure to Teratogens
Drugs such as warfarin, retinoic acid, lithium, anticonvulsants, angiotensin-converting enzyme (ACE) inhibitors, selective serotonin reuptake inhibitors, alcohol, prostaglandin synthetase inhibitors (eg, ibuprofen or salicylic acid), as well as infections (rubella, parvovirus, coxsackievirus) and high doses of ionizing radiation are considered to place the fetus at risk for development of CHD.
Ultrasound Findings
Increased nuchal translucency, suspicious OB scan, and echogenic foci5,6 also warrant fetal echocardiographic examination.
Timing of Fetal Echocardiography
With the advances in techniques, fetal cardiac images can be obtained as early as 15 weeks gestation with transabdominal ultrasound, although the commonly accepted timing for an optimal fetal echocardiography is between 18 and 22 weeks.6
Equipment
Fetal ultrasound transducers must be in the range of 3 to 8 MHz transmitted frequency and may be sector or linear array.7 With wider near-field view, curvilinear probes may be more helpful.6 Frame rates of 80 to 100 Hz are needed to scan the fetal hearts, which have high heart rates. Throughout the examination, both lower and higher frequencies should be used to obtain the best acquisition possible. At lower frequencies, the system will have better tissue penetration. The tissue resolution will be lower, but the Doppler and color flow will give better recordings.4 In addition to detailed two-dimensional (2D) imaging, M-Mode, Doppler, color-flow Doppler, and image enlarging should be used during fetal cardiac scanning.7 Newer techniques of tissue Doppler imaging and three-dimensional (3D) imaging/reconstruction are also used as an adjunct in many centers.
Fetal Ultrasound Techniques
2D Imaging
Perhaps the most important part of fetal cardiac imaging is the 2D imaging in which the computer processes the sound waves that reflect back from structures and show us pictures of structures in a fan-like display. This is the primary modality that shows the structures in detail (walls, valves, myocardium, vessels, chambers, etc.) and lets the operator measure dimensions and function.
Doppler and Color Flow Imaging
A stationary source of sound produces a given pitch or frequency. If the sound is moving toward a recorder (transducer), the pitch appears increased, and if the sound is moving away from a recorder (transducer), the pitch appears decreased. This can be applied to the blood flow and the velocity of the flow. Conventionally, when the flow is toward the transducer, the color image encountered will be red, and when the flow is away from the transducer, the Doppler will be blue. This helps the operator identify the direction of the flow. When the blood cells move together with the same velocity, the flow will be laminar and usually one color. When there is an increase in flow velocity, as in valvar stenosis, the flow will be turbulent and will show many different colors at a point within that cardiac cycle. In addition to color flow Doppler identification of valvar stenosis or vascular narrowing, with pulsed-wave Doppler imaging, the velocity of the flow can be calculated. Since the velocities are generally low, pulsed-wave Doppler is the frequently used modality in fetal cardiac examination.4 Using the simplified Bernoulli’s principle, P = 4V2, where V is the measured velocity of the flow, calculations of flow gradients or intracardiac/intravascular pressure estimations can be made (see Chapter 11 for a more detailed explanation of Doppler imaging).
Fetal Cardic Examination
Complete fetal cardiac examination in an uncomplicated patient can be performed in 30 to 60 minutes. The scan should include but not be limited to examination of the following:7
- Fetal number
- Biparietal diameter (BPD) for estimation of gestational age
- Fetal lie and position
- Fetal visceral situs
- Cardiac position, cardiac axis
- Four-chamber anatomy
- Great vessels and their relationships
- Atrioventricular and semilunar valves
- Aortic and ductal arches
- Shunting at the foramen ovale (FO) and ductus
- Systemic and pulmonary veins
- Cardiac chamber dimensions/cardiothoracic index
- Cardiac systolic and diastolic function
- Wall thicknesses
- Valve/vessel dimensions
- Fetal heart rate and rhythm
- Umbilical cord and ductus venosus
- Pericardial and extracardiac spaces for fluid accumulation.
In addition to 2D images from 4-chamber view, 5-chamber view, long-axis views (LVOTs and RVOTs), short-axis view/sweep (3-vessel view), caval long-axis view, and ductal arch and aortic arch views, along with systematic Doppler examination of atrioventricular and semilunar valves, systemic and pulmonary veins, ductus venosus, FO, ductus arteriosus, aortic arch, and umbilical vessels should be a part of routine fetal cardiac examination.6,7
Although it is often not very easy to follow a sequence of scanning secondary to fetal (eg, fetal lie) and maternal (eg, obesity, previous intra-abdominal surgery) factors, every effort should be made to evaluate the fetal heart according to the above-recommended sequence.
In an OB fetal ultrasound examination, at least a 4-chamber heart along with 5-chamber view, outflow tracts with crossing over of the great vessels, and aortic and ductal arches should be visualized. The 3-vessel view will also be an added asset in determination of fetal cardiac abnormalities. In this way, most of the cardiac abnormalities will be seen or suspected to have the patient evaluated in detail by a fetal echocardiographer.7
Fetal Biometry, Fetal Position, Situs, Cardiac Axis, Cardiac Position, Heart Size, and Umbilical Cord
In order to correlate cardiac measurements and fetal growth, certain measurements are used for estimation of fetal gestational age. Fetal femur length, BPD, and head circumference are the most frequently used parameters (Figure 4I.1).

Figure 4I.1. Biparietal diameter. For estimation of gestational age, BPD is measured.
In addition, umbilical artery and venous Doppler interrogation should be a part of the fetal examination, since they can point out fetal hemodynamic compromise, especially in cases with TTTS, intrauterine growth retardation (IUGR), and hydrops (Figure 4I.2).
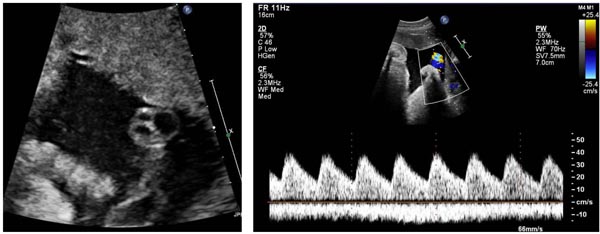
Figure 4I.2. Umbilical artery and vein Doppler. There are two umbilical arteries and one vein. Doppler interrogation under normal hemodynamic circumstances shows pulsatile flow in the umbilical artery in systole and continuation into diastole (above the baseline) and continuous flow (below the baseline) in the umbilical vein.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


