SWS is predominant during the first third of the sleep cycle, these disorders are more prevalent in the beginning of the night and are common in childhood— usually decreasing in frequency with increasing age (11,12). Arousal disorders may be triggered by a variety of conditions including fever, alcohol use, sleep deprivation, emotional stress, or medications. These precipitators should be viewed as triggering events in susceptible individuals rather than causal. A variety of primary sleep disorders such as obstructive sleep apnea (OSA) may also provoke disorders of arousal (13).
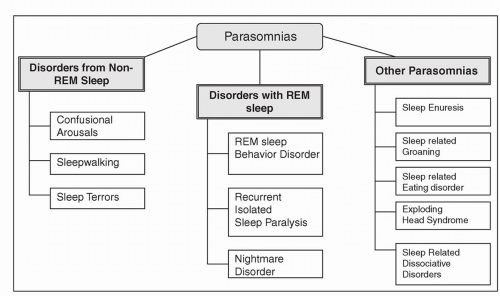 FIGURE 5.1 International Classifications of Sleep Disorders (ICSD)-2 for parasomnias. Disorders from Non-REM sleep are also known as disorders of arousal. Parasomnias categorized as “other parasomnias” do not show a strong predilection for NREM or REM sleep. Non-REM, “non rapid eye movement”; REM, “rapid eye movement.” (Modified from: Avidan AY, Kaplish N. The parasomnias: epidemiology, clinical features, and diagnostic approach. Clin Chest Med. Jun 2010;31(2):353-370.) |
CNS depressants (i.e., hypnotics, sedatives, tranquilizers, alcohol, and antihistamines); and underlying metabolic, hepatic, renal, and toxic encephalopathies. Confusional arousals are often seen in conditions characterized with pathologic hypersomnia, such as in patients with narcolepsy or OSA. Episodes of confusional arousals are frequent in patients with sleep terrors and sleepwalking. Organic causes of confusional arousals are rare but may include lesions in arousal generators, such as the periventricular gray, the midbrain reticular area, and the posterior hypothalamus.
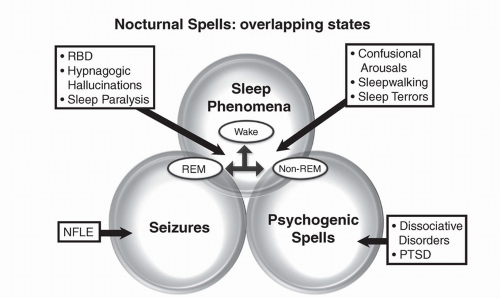 FIGURE 5.2 According to a model described by Mahowald & Schenck, parasomnias are explainable on the basic notion that that sleep and wakefulness are not mutually exclusive states but may dissociate and oscillate rapidly. The abnormal admixture of the three states of being (overlapping states of being)-Non-REM sleep, REM sleep, and wakefulness- may overlap, giving rise to parasomnias. REM parasomnias occur due to the abnormal intrusion of wakefulness into REM sleep, and likewise non-REM parasomnias such as sleep walking occur due to abnormal intrusions of wakefulness into Non-REM sleep. Other nocturnal spells that may be confused with parasomnias include nocturnal frontal lobe epilepsy (NFLE) and psychogenic spells such as post traumatic stress disorder (PTSD) and dissociative disorders. (Modified after Mahowald MW, Schenck CH. Non-rapid eye movement sleep parasomnias. Neurol Clin. Nov 2005;23(4):1077-1106, vii). |
TABLE 5.1 Key Similarities and Differentiating Features Between Non-REM and REM Parasomnias as Well as Nocturnal Seizures | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1. Sleep terrors are differentiated by symptoms of acute autonomic hyperarousal and fear.
2. Sleepwalking includes ambulation and complex motor automatisms.
3. RBD consists of dream enactment and complex movements such as fighting and punching while asleep in older male patients.
4. Sleep-related epileptic seizures of the partial complex type with confusional automatisms are rare, are diurnal, and associated with an epileptic EEG pattern.
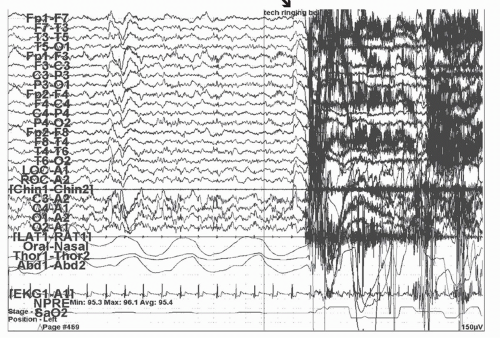 FIGURE 5.3 Confusional arousal clinical vignette. 37 year old man with a history of shift work disorder (SWD) presented to the sleep disorders clinic complaining of unusual nocturnal spells. This is an example from the patient’s PSG which utilized expanded EEG montage and esophageal pressure monitoring (for the evaluation of upper airway resistance). The nighttime sleep techs sounded an alarm at 4 AM which coincided with the timing of his typical spells, in the hope of inducing one. The figure is representative from the recorded episode when the alarm was sounded (  = “tech ringing bell”) during which he had an arousal form stage N2 sleep accompanied by confusion, disorientation and complete amnesia for the event in the morning. This event and the clinical history in the absence of epileptiform activity during the study or another comorbid sleep disorder was most suggestive of confusional arousal which resolved after the patient improved his sleep hygiene. = “tech ringing bell”) during which he had an arousal form stage N2 sleep accompanied by confusion, disorientation and complete amnesia for the event in the morning. This event and the clinical history in the absence of epileptiform activity during the study or another comorbid sleep disorder was most suggestive of confusional arousal which resolved after the patient improved his sleep hygiene. |
1. Sleep terrors: Sleepwalking episodes are distinguished from sleep terrors in that the latter are often accompanied with an attempt to “escape” from the terrifying stimulus and have an associated autonomic hyperarousal, such as fear, and panic coupled with a scream and aggression (Fig. 5.4).
2. RBD: RBD is characterized clinically based on episodes during REM sleep of complex dream-enactment, fragmentary recall, and abnormal augmentation of muscle activity.
3. Sleep-related epilepsy with ambulatory automatism: Can be distinguished by an epileptiform EEG.
4. Nocturnal eating syndrome: Characterized by ambulatory behavior of eating.
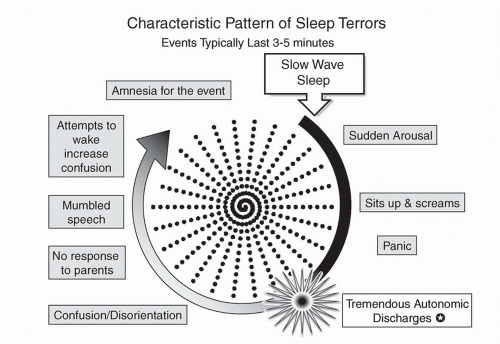 FIGURE 5.4 Characteristic pattern of sleep terror. Sleep terrors are characterized by a sudden arousal associated with a scream, agitation, panic and heightened autonomic activity  . Inconsolability is almost universal. The child is incoherent and has altered perception of the environment, appearing confused. This behavior may potentially be dangerous and could result in injury. (Modified from: Avidan AY, Kaplish N. The parasomnias: epidemiology, clinical features, and diagnostic approach. Clin Chest Med. Jun 2010;31(2):353-370.) . Inconsolability is almost universal. The child is incoherent and has altered perception of the environment, appearing confused. This behavior may potentially be dangerous and could result in injury. (Modified from: Avidan AY, Kaplish N. The parasomnias: epidemiology, clinical features, and diagnostic approach. Clin Chest Med. Jun 2010;31(2):353-370.) |
TABLE 5.2 Differences Between Sleep Terrors and Nightmares | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
1. Nightmares: Differentiation from nightmares is most important (Table 5.2). Sleep terrors are characterized by amnesia of the event compared to the vivid recollection in patients with nightmares. Nightmares also occur during the last third of the night, but unlike sleep terrors, they are confined to REM sleep. Associated with a vivid recollection and normal cognition, nightmares usually lack the sympathetic activation and confusion that is frequent with sleep terrors.
2. Confusional arousals: Are awakenings from SWS without terror or ambulation.
3. Sleep-related epilepsy: Episodes tend to be more frequent, occur several times per night, and have ictal abnormalities on the PSG/EEG recordings.
4. OSA: Patients to have phenotypic evidence of crowded airways, snoring, and evidence of apneic episodes associated with oxygen desaturations on PSG.
to 5 have clinically significant nightmares that disturb their parents. Up to 75% of the population can remember at least one or a few nightmares in the course of their childhood. About half of adults admit to having an occasional nightmare. About 1% of the adult population is afflicted with frequent nightmares of more than one per week. Nightmares usually start at age 3 to 6 years but can occur at any age. In children, the gender ratio is equal, while in adults there is a male: female ratio of 1:2 to 1:4 favoring females.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


