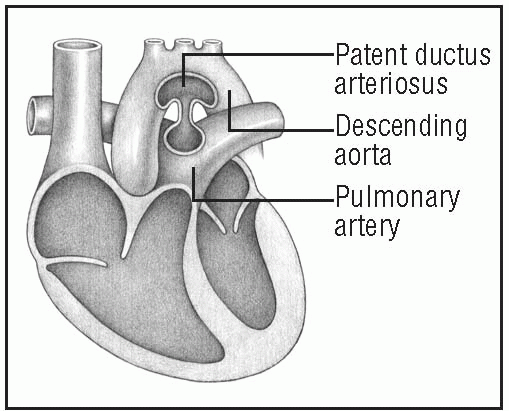
The ductus arteriosus is a fetal blood vessel connecting the pulmonary artery to the descending aorta, just distal to the left subclavian artery. During fetal development, the ductus directs blood from the right ventricle away from the fetus’s fluid-filled lungs. Normally, the ductus closes within days after birth.
In patent ductus arteriosus (PDA), the lumen of the ductus remains open after birth. (See Understanding patent ductus arteriosus, page 148). This creates a left-to-right shunt of blood from the aorta to the pulmonary artery and results in recirculation of arterial blood through the lungs. Initially, PDA may produce no clinical effects. In time, however, it can cause pulmonary vascular disease, causing symptoms to appear by age 40. The prognosis is good if the shunt is small or surgical repair is effective. Otherwise, PDA may advance to intractable heart failure, which may be fatal.
CAUSES AND INCIDENCE
Normally, the ductus closes within days to weeks after birth. Failure to close is most prevalent in premature neonates, probably as a result of abnormalities in oxygenation or the relaxant action of prostaglandin E, which prevents the ductal spasm and contracture needed for closure. PDA commonly accompanies rubella syndrome and may be linked to other congenital defects, such as coarctation of the aorta, ventricular septal defect, and pulmonary and aortic stenoses.
The ductus arteriosus normally closes as prostaglandin levels from the placenta fall and oxygen levels rise. This process typically begins as soon as the neonate takes its first breath but may take as long as 3 months in some children.
In PDA, relative resistances in pulmonary and systemic vasculature and the size of the ductus determine the amount of left-to-right shunting. Because of increased aortic pressure, oxygenated blood is shunted from the aorta through the ductus arteriosus to the pulmonary artery. The blood returns to the left side of the heart and is pumped out to the aorta once more.
The left atrium and left ventricle must accommodate the increased pulmonary venous return, which increases filling pressure and workload on the left side of the heart, possibly causing heart failure. In the final stages of untreated PDA, the left-to-right shunt leads to chronic pulmonary artery hypertension that becomes fixed and unreactive. This causes the shunt to reverse; unoxygenated blood thus enters systemic circulation, causing cyanosis.
UNDERSTANDING PATENT DUCTUS ARTERIOSUS
This anomaly occurs when the ductus arteriosus—a tubular connection that shunts blood away from the fetal pulmonary circulation —fails to close after birth. Blood then shunts from the aorta to the pulmonary artery.
PDA is found in 1 of every 2,500 to 5,000 infants and is the most common congenital heart defect in adults. It affects twice as many females as males.
SIGNS AND SYMPTOMS
In neonates, especially those who are premature, a large PDA usually produces respiratory distress and signs of heart failure from the tremendous volume of blood shunted to the lungs through a patent ductus and the increased workload on the left side of the heart. Other characteristic features may include heightened susceptibility to respiratory tract infections, slow motor development, and failure to thrive.
Most children with PDA have no symptoms except cardiac ones. Others may show signs of heart disease, such as physical underdevelopment, fatigability, and frequent respiratory tract infections. Adults with undetected PDA may develop pulmonary vascular disease and, by age 40, may have fatigability and dyspnea on exertion. About 10% of them develop infective endocarditis.
Auscultation reveals the classic machinery murmur (Gibson murmur) in 85% of children with PDA. This is a continuous murmur (during systole and diastole) best heard at the heart’s base, at the second left intercostal space under the left clavicle. The murmur may obscure S2. (See Auscultating for patent ductus arteriosus.) However, with a right-to-left shunt, such a murmur may be absent.
Palpation may reveal a thrill at the left sternal border and a prominent left ventricular impulse. Peripheral arterial pulses are bounding (Corrigan’s pulse); pulse pressure will be widened because of a drop in diastolic blood pressure and, secondarily, a rise in systolic pressure.
COMPLICATIONS
Left-sided heart failure
Pulmonary artery hypertension
Respiratory distress (children)
Infective endocarditis
Recurrent pneumonia
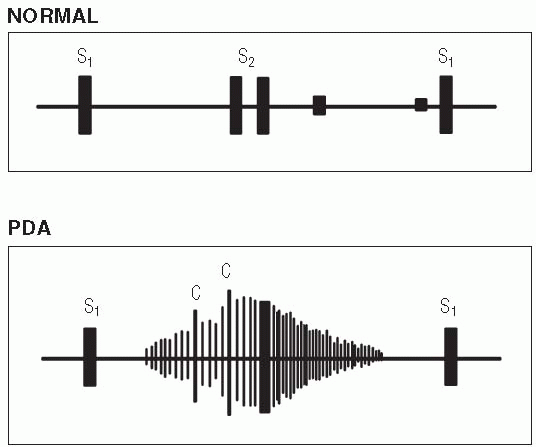
AUSCULTATING FOR PATENT DUCTUS ARTERIOSUS
To detect patent ductus arteriosus (PDA), auscultate the base of the heart at the second left intercostal space under the left clavicle. You’ll hear systolic clicks (C) and a continuous murmur during systole and diastole, possibly not through the entire cycle but through S2 in a crescendo-decrescendo manner, as shown below.
DIAGNOSIS
• Chest X-ray may show increased pulmonary vascular markings, prominent pulmonary arteries, and left ventricle and aorta enlargement.
• Electrocardiograph (ECG) may be normal or may indicate left atrial or ventricular hypertrophy and, in pulmonary vascular disease, biventricular hypertrophy.
• Echocardiography detects and helps estimate the size of a PDA. It also reveals an enlarged left atrium and left ventricle or right ventricular hypertrophy from pulmonary vascular disease.
• Cardiac catheterization shows pulmonary arterial oxygen content higher than right ventricular content because of the influx of aortic blood. Increased pulmonary artery pressure indicates a large shunt or, if it exceeds systemic arterial pressure, severe pulmonary vascular disease. Catheterization allows calculation of blood volume crossing the ductus and can rule out associated cardiac defects. Dye injection definitively demonstrates PDA.
TREATMENT
Asymptomatic infants with PDA need no immediate treatment. Those with heart failure need fluid restriction, diuretics, and cardiac glycosides to minimize or control symptoms. If these measures can’t control heart failure, surgery is needed to ligate the ductus. Surgery can be performed via a left thoracotomy or visual assisted thoracoscopic surgery (VATS). VATS may be done at the bedside or in a procedure room. This technique involves three small incisions on the left side of the chest through which a clip is placed on the ductus. If symptoms are mild, surgical correction is usually delayed until the infant is between ages 6 months and 3 years, unless problems develop. Other options include a cardiac catheterization to deposit a plug (or “umbrella”) or coils in the ductus to stop shunting.
Drugs
• Indomethacin (Indocin) to induce ductus spasm and closure in premature infants
• A prophylactic antibiotic to protect against infective endocarditis
• Diuretic and digoxin (Lanoxin) to treat heart failure
SPECIAL CONSIDERATIONS
• PDA requires careful monitoring, patient and family teaching, and emotional support.
• Watch carefully for signs of PDA in all premature neonates.
• Be alert for respiratory distress symptoms resulting from heart failure, which may develop rapidly in a premature neonate. Assess vital signs, ECG, electrolyte levels, and intake and output. Record the patient’s response to diuretics and other therapy. Watch for evidence of digoxin toxicity, such as poor feeding and vomiting.
• If the infant receives indomethacin for ductus closure, watch for possible adverse effects, such as diarrhea, jaundice, bleeding, and renal dysfunction.
• Before surgery, carefully explain all treatments and tests to parents. Include the child in your explanations. Arrange for the child and her parents to meet the intensive care unit staff. Tell them about expected I.V. lines, monitoring equipment, and postoperative procedures.
• Immediately after surgery, the child may have a central venous pressure catheter and an arterial line in place. Carefully assess vital signs, intake and output, and arterial and venous pressures. Provide pain relief as needed.
• Before discharge, review instructions to the parents about activity restrictions based on the child’s tolerance and energy levels. Advise parents not to become overprotective as their child’s tolerance for physical activity increases.
• Stress the need for regular followup examinations. Advise parents to inform any practitioner who treats their child about her history of surgery for PDA—even if the child is being treated for an unrelated medical problem.
Pericarditis
Pericarditis is an inflammation of the pericardium, which is the fibroserous sac that envelops, supports, and protects the heart. The disorder may be acute or chronic. Acute pericarditis can be fibrinous or effusive, with purulent serous or hemorrhagic exudates. Chronic constrictive pericarditis is characterized by dense fibrous pericardial thickening. The prognosis depends on the underlying cause and usually is good in acute pericarditis, unless constriction occurs.
CAUSES AND INCIDENCE
Common causes of this disease include bacterial, fungal, or viral infection (infectious pericarditis); neoplasms (primary or metastatic from lungs, breasts, or other organs); high-dose radiation to the chest; uremia; hypersensitivity or autoimmune disease, such as acute rheumatic fever (most common cause in children), systemic lupus erythematosus, and rheumatoid arthritis; postcardiac injury such as myocardial infarction (MI), which later causes an autoimmune reaction (Dressler’s syndrome) in the pericardium; trauma or surgery that leaves the pericardium intact but causes blood to leak into the pericardial cavity; drugs, such as hydralazine (Apresazide), procainamide, isoniazid (Nydrazid), cyclosporine (Gengraf), or tetracyclines; and idiopathic factors (most common in acute pericarditis).
Less common causes include aortic aneurysm with pericardial leakage and myxedema with cholesterol deposits in the pericardium.
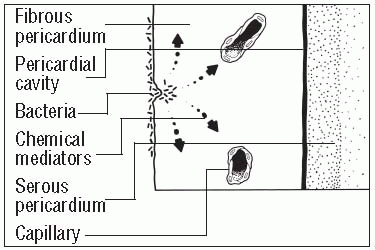
Pericardial tissue damaged by bacteria or other substances results in the release of chemical mediators of inflammation (prostaglandins, histamines, bradykinins, and serotonin) into the surrounding tissue, thereby initiating the inflammatory process. Friction occurs as the inflamed pericardial layers rub against each other. Histamines and other chemical mediators dilate vessels and increase vessel permeability. Vessel walls then leak fluids and protein (including fibrinogen) into tissues causing extracellular edema. Macrophages already present in the tissue begin to phagocytize the invading bacteria and are joined by neutrophils and monocytes. After several days, the area fills with an exudate composed of necrotic tissue and dead and dying bacteria, neutrophils, and macrophages. Eventually the contents of the cavity autolyze and are gradually reabsorbed into healthy tissue. (See Understanding pericarditis, page 152).
A pericardial effusion develops if fluid accumulates in the pericardial cavity. Cardiac tamponade results when fluid accumulates rapidly in the pericardial space, compressing the heart, preventing it from filling during diastole, and reducing cardiac output.
Chronic constrictive pericarditis develops if the pericardium becomes thick and stiff from chronic or recurrent pericarditis, encasing the heart in a stiff shell and preventing it from properly filling during diastole. This causes an increase in left- and right-sided filling pressures, leading to a drop in stroke volume and cardiac output.
UNDERSTANDING PERICARDITIS
Pericarditis occurs when a pathogen or other substance attacks the pericardium, leading to the following events.
Inflammation
Pericardial tissue damaged by bacteria or other substances releases chemical mediators of inflammation (such as prostaglandins, histamines, bradykinins, and serotonins) into the surrounding tissue, starting the inflammatory process. The inflamed pericardial layers rub against each other, creating friction.
Vasodilation and clotting
Histamines and other chemical mediators cause vasodilation and increased vessel permeability. Local blood flow (hyperemia) increases. Vessel walls leak fluids and proteins (including fibrinogen) into tissues, causing extracellular edema. Clots of fibrinogen and tissue fluid form a wall, blocking tissue spaces and lymph vessels in the injured area. This wall prevents the spread of bacteria and toxins to adjoining healthy tissues.
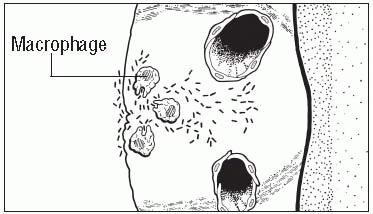
Initial phagocytosis
Macrophages already present in the tissues begin to phagocytize the invading bacteria but usually fail to stop the infection.
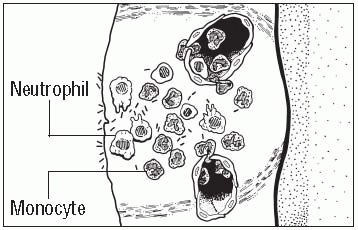
Enhanced phagocytosis
Substances released by the injured tissue stimulate neutrophil production in the bone marrow. Neutrophils then travel to the injury site through the bloodstream and join macrophages in destroying pathogens. Meanwhile, additional macrophages and monocytes migrate to the injured area and continue phagocytosis.
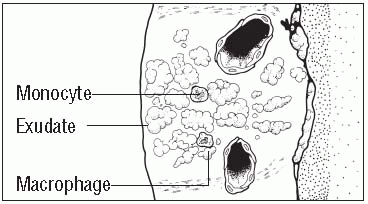
Exudation
After several days, the infected area fills with an exudate composed of necrotic tissue and dead and dying bacteria, neutrophils, and macrophages. This exudate, which is thinner than pus, forms until all infection ceases, creating a cavity that remains until tissue destruction stops. The contents of the cavity autolyze and are gradually reabsorbed into healthy tissue.
Fibrosis and scarring
As the end products of the infection slowly disappear, fibrosis and scar tissue may form. Scarring, which can be extensive, can ultimately cause heart failure if it restricts movement.
Pericarditis most commonly affects men ages 20 to 50, but it can also occur in children following infection with an adenovirus or coxsackievirus.
SIGNS AND SYMPTOMS
Acute pericarditis usually produces a sharp, sudden pain that starts over the sternum and radiates to the neck, shoulders, back, and arms. However, unlike the pain of MI, pericardial pain often is pleuritic, increasing with deep inspiration and decreasing when the patient sits up and leans forward, pulling the heart away from the diaphragmatic pleurae of the lungs.
Pericardial friction rub, a classic sign, is a grating sound heard as the heart moves. Usually, it can best be auscultated during forced expiration, while the patient leans forward or is on his hands and knees in bed. It may have up to three components, corresponding to the timing of atrial systole, ventricular systole, and the rapid-filling phase of ventricular diastole. Occasionally, this friction rub is heard only briefly or not at all.
Pericardial effusion, the major complication of acute pericarditis, may produce effects of heart failure (such as dyspnea, orthopnea, and tachycardia), ill-defined substernal chest pain, and a feeling of fullness in the chest. (See Patterns of cardiac pain, page 154.) If acute pericarditis has caused very large pericardial effusions, physical examination reveals increased cardiac dullness and diminished or absent apical impulse and distant heart sounds.
Chronic constrictive pericarditis causes a gradual increase in systemic venous pressure and produces symptoms similar to those of chronic right-sided heart failure (fluid retention, ascites, and hepatomegaly).
PATTERNS OF CARDIAC PAIN
Although everyone feels the effects of cardiac disorders uniquely, the disorders listed here tend to produce certain kinds of pain.
Cause
Onsetand duration
Location and radiation
Quality and intensity
Signs and symptoms
Precipitating factors
Pericarditis
▪ Sudden onset
▪ Continuous pain lasting days
▪ Residual soreness
▪ Substernal pain to left of midline
▪ Radiation to back or subclavicular area
▪ Mild ache to severe pain
▪ Deep or superficial
▪ May be described as stabbing or knifelike
▪ Precordial friction rub
▪ Increased pain with movement, inspiration, laughing, coughing
▪ Decreased pain with sitting or leaning forward (which pulls heart away from diaphragm)
▪ Myocardial infarction
▪ Upper respiratory tract infection
▪ Invasive cardiac trauma
Angina
▪ Gradual or sudden onset
▪ Pain usually lasting less than 15 and no more than 30 minutes (average, 3 minutes)
▪ Substernal or anterior chest pain
▪ Not sharply localized
▪ Radiation to back, neck, arms, jaw, even upper abdomen or fingers
▪ Mild to moderate pressure
▪ Deep sensation
▪ Varied pattern of attacks
▪ May be described as tightness, squeezing, crushing, pressure
▪ Dyspnea
▪ Diaphoresis
▪ Nausea
▪ Desire to void
▪ Belching
▪ Apprehension
▪ Exertion
▪ Stress
▪ Eating
▪ Cold weather
▪ Hot, humid weather
Myocardial infarction
▪ Sudden onset
▪ Pain lasting 30 minutes to 2 hours
▪ Waxes and wanes
▪ Residual soreness for 1 to 3 days
▪ Substernal, midline, or anterior chest pain
▪ Radiation to jaw, neck, back, shoulders, or one or both arms
▪ Persistent, severe pressure
▪ Deep sensation
▪ May be described as crushing, squeezing, heavy, oppressive
▪ Nausea, vomiting
▪ Apprehension
▪ Feeling of impending doom
▪ Dyspnea
▪ Diaphoresis
▪ Increased or decreased blood pressure
▪ Gallop heart sound
▪ Physical exertion
▪ Emotional stress
▪ May occur at rest
COMPLICATIONS
Pericardial effusion
Constrictive pericarditis
Cardiac tamponade
Shock
Cardiovascular collapse
Death
DIAGNOSIS
• Diagnosis includes typical clinical features and elimination of other possible causes.
• Chest X-ray, echocardiogram, magnetic resonance imaging of the chest and heart, computed tomography scan of the heart, and radionuclide scanning can detect fluid that has accumulated in the pericardial sac. They may also show enlargement of the heart and signs of inflammation or scarring, depending on the cause of pericarditis. In pericardial effusion, echocardiography is diagnostic when it shows an echofree space between the ventricular wall and the pericardium.
• Laboratory results reflect inflammation and may identify its cause. They may include a normal or elevated white blood cell count, especially in infectious pericarditis, an elevated erythrocyte sedimentation rate, and slightly elevated cardiac enzyme levels with associated myocarditis. Culture of pericardial fluid obtained by open surgical drainage or cardiocentesis sometimes identifies a causative organism in bacterial or fungal pericarditis.
• Electrocardiography shows the following changes in acute pericarditis: elevation of ST segments in the standard limb leads and most precordial leads without the significant changes in QRS morphology that occur with MI, atrial ectopic rhythms such as atrial fibrillation and, in pericardial effusion, diminished QRS voltage.
• Blood urea nitrogen levels are used to check for uremia.
• A purified protein derivative skin test may be used to check for tuberculosis.
TREATMENT
The goal of treatment is to relieve symptoms and manage the underlying systemic disease. In acute idiopathic pericarditis and postthoracotomy pericarditis, treatment includes nonsteroidal anti-inflammatory drugs (NSAIDs) and bed rest as long as fever and pain persist. If NSAIDs fail to relieve symptoms, corticosteroids may be used. Post-MI patients should avoid NSAIDs and steroids because they may interfere with myocardial scar formation.
Infectious pericarditis that results from disease of the left pleural space, mediastinal abscesses, or septicemia requires antibiotics (possibly by direct pericardial injection), surgical drainage, or both. Pericardiocentesis, guided by echocardiography, is the technique used to drain the effusion.
Recurrent pericarditis may require partial pericardectomy to create a window through which fluid can drain into the pleural space. In constrictive pericarditis, the patient may need total pericardectomy to permit adequate filling and contraction of the heart. Treatment also must include management of rheumatic fever, uremia, tuberculosis, and other underlying disorders.
Only gold members can continue reading. Log In or Register to continue