duplicate arteries can potentially decrease the sensitivity of noninvasive testing (pressure measurements and plethysmographic waveforms) in identifying UEAD. For example, normal forearm and digital pressures as well as pulsed volume recording (PVR) waveforms may be obtained in the setting of an occluded ulnar artery.
TABLE 16.1 CLASSIFICATION SCHEME FOR UPPER EXTREMITY ARTERIAL DISEASE | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
digital perfusion intermittently ceases. Physiological vasospasm is never associated with complete cessation of digital perfusion. Primary Raynaud’s syndrome only involves functional alterations, whereas secondary Raynaud’s syndrome also involves associated structural microvascular abnormalities. The pathogenesis of Raynaud’s syndrome includes defects in one of more of these three systems: (a) vascular (endothelial dysfunction; structural defects), (b) neural (central dysfunction; impaired vasodilation; impaired vasoconstriction), and (c) intravascular abnormality (increased platelet activation and aggregation; impaired fibrinolysis).
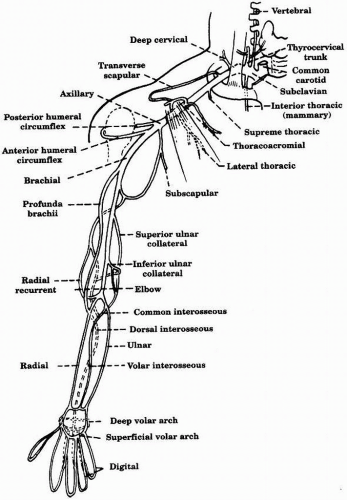 FIGURE 16-1. Arterial supply of the upper extremity. |
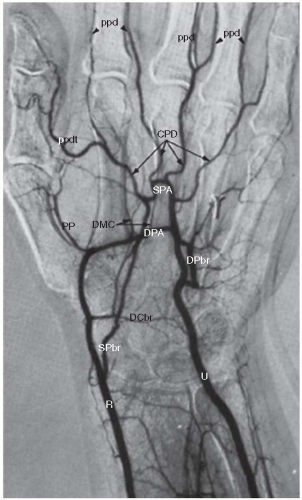 FIGURE 16-2. Normal arteriogram of the hand showing the arches (superficial and deep). (CPD, common palmar digital; DCbr, dorsal carpal branch; DMC, dorsal metacarpal; DPA, deep palmar arch; DPbr, deep palmar branch of ulnar; PP, princeps pollicis (main artery to the thumb); ppd, palmar proper digital; ppdt, palmar proper digital thumb; R, radial; SPA, superficial palmar arch; SPbr, superficial palmar branch of radial; U, ulnar.) (Adapted from Kadir S. Atlas of normal and variant angiographic anatomy. W. B. Saunders Company, 1991.) |
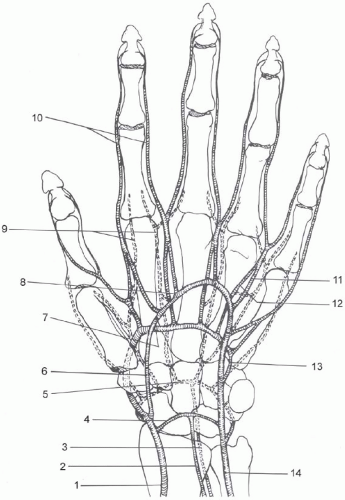 FIGURE 16-3. Arterial anatomy of the hand. (1, Radial; 2, Anterior interosseus; 3, Posterior interosseus; 4, Palmar carpal branch; 5, Dorsal carpal branch forming the dorsal carpal rete; 6, Superficial palmar branch of the radial artery; 7, Deep palmar arch; 8, Superficial palmar arch; 9, Dorsal metacarpal arteries; 10, Proper palmar digital arteries; 11, Common palmar digital arteries; 12, Palmar metacarpal; 13, Deep palmar branch of the ulnar artery; 14, Ulnar artery.) (Adapted from Kadir S. Atlas of normal and variant angiographic anatomy. W. B. Saunders Company, 1991.) |
TABLE 16.2 ARTERIAL VARIANTS OF THE UPPER EXTREMITY | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||



