Overview of Congenital Heart Disease
The excellent results obtained in infants and children using transthoracic echocardiography limit the need to use the transesophageal approach to elucidate lesions of congenital heart disease. In some patients, however, it is not possible to perform adequate transthoracic studies, particularly in adults with congenital heart disease. Furthermore, transesophageal echocardiography is the only practical method for assessing operative results during the procedure.
The septum primum covers the septum secundum and closes the fossa ovalis. In about 25% of patients this coverage is not complete, and a flow may occur across the septum. This is particularly likely in the setting of elevated right-sided pressures, which can open the patent foramen and result in paradoxic embolus. The secundum defect occurs at the level of the fossa ovalis and is the commonest of atrial septal defects. These lesions often present as a single large defect but may be fenestrated or multiple. Defects <2 cm in diameter can be closed by transcatheter patch closure, but larger defects must be closed surgically. The size of the defect is easily assessed by transesophageal echocardiography, especially if the multiplane probe is used.
The ostium primum type of atrial septal defect (partial atrioventricular septal defect or partial atrioventricular canal defect) occurs at the base of the septum. It is often associated with a cleft in the anterior mitral valve leaflet that makes it regurgitant. In contrast, sinus venosus atrial septal defects occur in the superior part of the septum. Drainage of the right upper pulmonary vein into the right atrium is a commonly associated anomaly. The superior vena cava may override the defect. In adults, this defect may be difficult to visualize by transthoracic echocardiography. When an atrial septal defect is suspected on the basis of other findings but is not found on transthoracic examination, transesophageal echocardiography is indicated.
Ventricular septal defects, especially small ones, are often visualized more effectively on transthoracic echocardiography than on transesophageal echocardiography because more planes are available from the transthoracic approach. Patent ductus arteriosus and other aortopulmonary communications, both congenital and surgically created, can be visualized by transesophageal echocardiography.
Stenosis of the pulmonary veins is usually diagnosed early. It can be seen as a narrowing of the vein, and Doppler examination demonstrates a high-velocity narrow jet with turbulence and spectral broadening. In adults, congenital stenosis must be differentiated from acquired narrowing produced by mediastinal lesions such as a tumor or sclerosing mediastinitis and pulmonary vein obstruction occurring after lung transplantation. In cor triatriatum, a membrane partitions the left atrium (or, rarely, the right atrium) into two chambers in such a way that the pulmonary veins are on one side of the membrane and the left atrial appendage is on the other side. Cor triatriatum is different from a supravalvar mitral membrane, which is located below and inferior to the left atrial appendage. These lesions may or may not result in obstruction to the flow. Congenital mitral stenosis is a rare lesion, similar in presentation to mitral stenosis. The valve is thickened and domes in diastole. Associated abnormalities of the papillary muscle and chordae may be present.
Subvalvular aortic stenosis results from a fibromuscular membrane that has a location that is variable relative to the aortic valve. These membranes are most commonly attached to the base of the anterior mitral leaflet and to the ventricular septum. Subvalvular membranes appear as linear echoes in the left ventricular outflow tract. Turbulent flow and a high gradient may be present, and there is often associated aortic regurgitation. Early, as opposed to
mid- or late, systolic closure of the aortic valve is commonly seen. It may involve only one cusp.
mid- or late, systolic closure of the aortic valve is commonly seen. It may involve only one cusp.
In congenital aortic stenosis the valve domes in systole. The short-axis view shows a typical “circle within a circle” appearance. Careful planimetry yields a good estimate of the valve area. Care must be taken to move the probe up and down the esophagus to visualize even the smallest flow-limiting orifice at the top of the domed valve. Color Doppler allows visualization of the width of the jet. A jet that is 7 mm or smaller suggests severe aortic stenosis in an adult. The jet width should be measured at its origin from the aortic valve. Color Doppler should be turned off during planimetry of the orifice because it tends to overestimate the area. It is, however, useful in identifying the aortic orifice in patients with heavily calcified valves that show no discernible opening movement in systole (i.e., fixed orifice). In these cases, the first appearance of turbulent flow signals in early systole helps identify the stenotic orifice, which can then be studied through planimetry with the color Doppler turned off. After valvotomy the jet size is larger, and the planimetered area is also greater. Because the transesophageal study can be performed intraoperatively, it is useful in guiding surgery. Supravalvular aortic stenosis is a rare lesion that may present as a discrete membrane or may be tubular. Coarctation of the aorta is best seen on transthoracic echocardiography but may also be evaluated by the transesophageal approach. The best results are obtained with a multiplane probe.
Membranes occur in the right atrium. Examples include eustachian valves and Chiari networks. Obstruction is rare but may occur. Right ventricular muscle bundles may be prominent and are associated with right ventricular hypertrophy. Rarely, the hypertrophy may be sufficient to cause obstruction in the body of the ventricle. A small ventricular septal defect may be associated, and it is suspected that the jet from the defect may, at least in some cases, stimulate hypertrophy. Infundibular stenosis may occur alone or in association with tetralogy of Fallot. The right ventricular outflow tract is best viewed in the long axis using longitudinal plane examination.
In congenital pulmonary stenosis the valve domes in systole and may also be thickened. Stenosis in the proximal segments of the right or left pulmonary arteries can be visualized by transesophageal echocardiography; however, stenosis in the distal segments or in the peripheral branches cannot be visualized using echocardiographic techniques.
The pathophysiologic features of complete atrioventricular canal defect (atrioventricular septal defect), including absence of the atrioventricular septum, deficiency of the adjacent atrial and inlet ventricular septum, a common atrioventricular annulus, and shunting from the left atrium into the right atrium and from the left ventricle into the right ventricle, are well seen using the transesophageal approach. The severity of atrioventricular valve regurgitation can also be evaluated.
In tricuspid atresia, the tricuspid valve is absent and both atrial and ventricular septal defects are necessarily present to ensure patient survival. This lesion is often associated with a hypoplastic right ventricle. For the purpose of surgical planning, it is necessary to delineate the right ventricular outflow tract, the pulmonary valve, and the pulmonary artery. Surgical correction (i.e., the Fontan procedure) involves closure of the atrial septal defect, closure of any ventricular septal defect, and placement of a shunt from the right atrium to the pulmonary artery.
In transposition of the great vessels, the connection of the vessels to the ventricles can be seen and the relation of the pulmonary artery and the aorta can be delineated. Associated pulmonary valve stenosis can be seen, as can banding of the pulmonary artery. Coexisting atrial or ventricular septal defects and atrioventricular or semilunar valve regurgitation can also be assessed by transesophageal echocardiography. The adequacy of the Mustard procedure can be assessed immediately after the operation. Intra-atrial baffle leak or obstruction can be delineated. In congenitally corrected transposition of the great vessels, the discordant atrioventricular and ventriculoarterial connections, together with the presence and degree of Ebsteinization of the left-sided atrioventricular valve, can be assessed by transesophageal echocardiography.
Ebstein anomaly is characterized by the apparent displacement of one or more tricuspid valve leaflets into the right ventricle, resulting from a variable extent and degree of plastering of the leaflets to the contiguous ventricular septum or right ventricular wall. The degree of this displacement determines the size of the functional right ventricle. Transesophageal echocardiography is useful in assessing both these abnormalities and the severity of tricuspid regurgitation, which is often considerable. A patent foramen ovale or an atrial septal defect may be present, and may result in right-to-left shunting and cyanosis because of increased right atrial pressure. The anatomic features and the flow patterns of other complicated lesions, such as tetralogy of Fallot, double outlet right ventricle, and single ventricle can also be assessed through the transesophageal approach.
Abnormalities of the coronary arteries can be seen well. These include aneurysms, thrombi, and anomalous origins and course of the coronary arteries.
An important lesion is the sinus of Valsalva aneurysm. It may appear as a tube-like structure protruding into the right ventricle or the right atrium. Rupture may result in shunting into the right ventricle or the right atrium.
In the first part of this chapter the most common shunt lesions are illustrated, followed by the obstructive lesions (both left-sided and right-sided), and, finally, the more complex congenital pathologies. The second and third parts of this chapter supplement the material shown in the first part and provide an enhanced understanding of the role of transesophageal echocardiography in the assessment of congenital cardiac lesions.
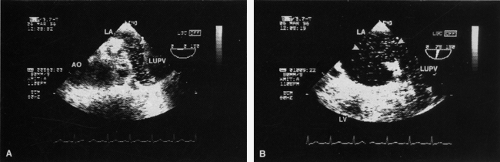 FIGURE 8.1.2. Right-to-left shunting in hepatopulmonary syndrome. A,B. Contrast echoes (arrowheads) appear in the left upper pulmonary vein (LUPV) following IV injection of normal saline. Contrast appeared in the pulmonary vein before appearing in the left atrium (LA), which indicates that the shunt is at the level of the pulmonary vasculature. This patient has hepatopulmonary syndrome resulting from cirrhosis. In this syndrome, the pulmonary capillaries are dilated, allowing the passage of contrast from the right to the left circulation. AO, aorta; LV, left ventricle. |
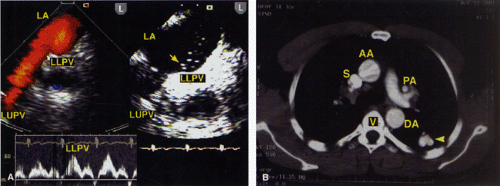 FIGURE 8.1.3. Contrast transesophageal echocardiographic detection of a pulmonary arteriovenous malformation draining into left lower pulmonary vein. A. Shows contrast echoes originating from the left lower pulmonary vein (LLPV) imaged in the longitudinal plane (L) examination. No contrast echoes are seen from the left upper pulmonary vein (LUPV), which is located further away from the probe as compared with LLPV. The left inset depicts pulsed Doppler spectral signals from LLPV. B. Computer tomography scan of the chest. The arrowhead points to the pulmonary arteriovenous malformation located in the lower lobe of the left lung. AA, ascending aorta; DA, descending thoracic aorta; L, longitudinal plane; LA, left atrium; PA, pulmonary artery; S, superior vena cava; V, vertebral body. (Reproduced with permission from Ahmed S, Navin C, Nekkanti R, et al. Contrast transesophageal echocardiographic detection of a pulmonary arteriovenous malformation draining into left lower pulmonary vein. Echocardiography 2003;20:391–394. ) |
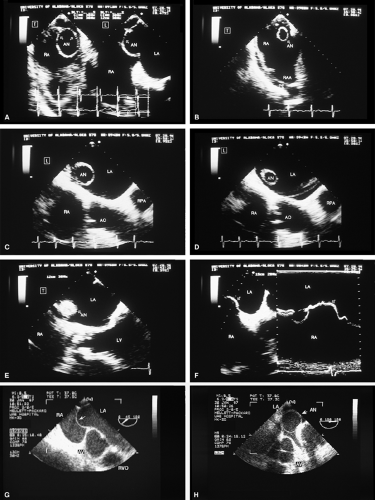 FIGURE 8.1.5. Atrial septal aneurysm. A. Biplane study shows the atrial septal aneurysm (AN) bulging into the right atrium (RA) during systole when examined in the longitudinal plane (right). In the transverse plane (left), the aneurysm appears as a circular structure in the short-axis view. B. Transverse plane imaging demonstrates the aneurysm in short axis as it bulges into the RA in systole, and its relation to the right atrial appendage (RAA). C,D. Longitudinal plane examination demonstrates the aneurysm bulging into the left atrium (LA) during diastole. E. In this view, the transverse plane skims the surface of the aneurysm, resulting in an erroneous appearance of a mass in the LA. F. M-mode examination shows the AN (arrow) bulging into the LA and into the RA during systole. The arrow in G and H shows another patient with an AN, which mimics an LA cyst in H. AO, aorta; AV, aortic valve; LV, left ventricle; PE, pericardial effusion; RPA, right pulmonary artery; RVO, right ventricular outflow tract. (A through F reproduced with permission from Zboyovsky KL, Nanda NC, Jain H. Transesophageal echocardiographic identification of atrial septal aneurysm. Echocardiography 1991;8:435–437. ) |
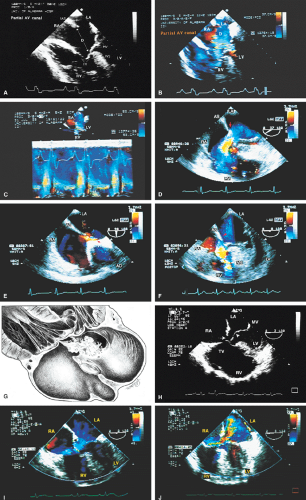 FIGURE 8.1.6. Partial atrioventricular septal (canal) defect. A–C. A large defect (D) is shown in the basal (inferior) portion of the atrial septum (AS) with no intact septum separating it from the attachment of the atrioventricular valves. B. Color Doppler examination demonstrates flow signals moving from the left atrium (LA) through the defect into the right atrium (RA), then through the open tricuspid valve (TV) into the right ventricle (RV). C. Color M-mode shows left-to-right shunting throughout the cardiac cycle except for a very small right-to-left component (dark red signals) occurring during the isovolumic relaxation period. D–F. Another patient with a partial atrioventricular canal defect. D. Left-to-right shunt (arrow) in the basal portion of the AS. E. An associated PFO (arrow). F. Patch closure (arrow) of the defect. Note the absence of shunting. G. Schematic demonstrates a large atrioventricular canal defect, an aneurysm of the membranous ventricular septum (VS), and mitral regurgitant flow passing through the defect into the RA. H–J. Another patient with partial atrioventricular canal defect. In H, the arrow points to the defect and the arrowhead to prolapse of the anterior mitral leaflet. I,J. Color Doppler examination shows left-to-right shunting (arrowhead in I) through the defect. AO, aorta; IVS, ventricular septum; LV, left ventricle; MV, mitral valve. (A reproduced with permission from Mehta RH, Helmcke F, Nanda NC, et al. Transesophageal Doppler color-flow mapping assessment of atrial septal defect. J Am Coll Cardiol 1990;16:1010–1016. ) |
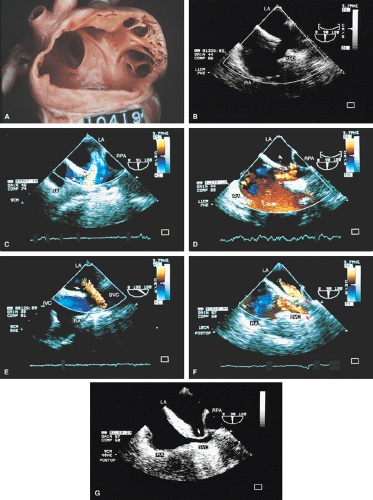 FIGURE 8.1.7. Sinus venosus atrial septal defect. A. Gross specimen shows a large sinus venosus atrial septal defect (ASD). B–E. A large defect is seen in the superior portion of the atrial septum, with flow signals (arrows) moving from the LA through the defect to the right atrium (RA) in C and from the RA to the left atrium (LA) in D. E. The superior vena cava (SVC) is seen straddling the atrial septum. Flow signals (arrow) are seen moving from the anomalous right upper pulmonary vein (RUPV) into the RA and then through the defect into the LA. F,G. Postoperative studies show the patch (upper arrow in F, arrow in G) used to close the defect. IVC, inferior vena cava; RPA, right pulmonary artery. |
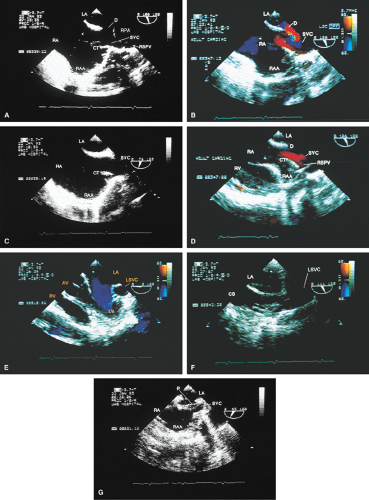 FIGURE 8.1.8. Sinus venosus atrial septal defect. A,B. Examination at a plane angulation of 106° demonstrates the defect (D) in the superior portion of the atrial septum. The entrance of superior vena cava (SVC) into the right atrium (RA) is identified by the presence of the prominent crista terminalis (CT). C. Examination at a plane angulation of 76° fails to reveal the presence of the defect in the superior portion of the atrial septum. D. Color Doppler examination at a plane angulation of 126° shows the right superior pulmonary vein (RSPV) entering the SVC near its entrance into the RA. This was confirmed at surgery. E,F. An associated left superior vena cava (LSVC) is seen entering an enlarged coronary sinus (CS) in F. G. The patch (P) used to close the defect. AV, aortic valve; LA, left atrium; LV, left ventricle; RAA, right atrial appendage; RPA, right pulmonary artery; RV, right ventricle. (Reproduced with permission from Maxted W, Finch A, Nanda NC, et al. Multiplane transesophageal echocardiographic detection of sinus venosus atrial septal defect. Echocardiography 1995;12:139–143. ) |
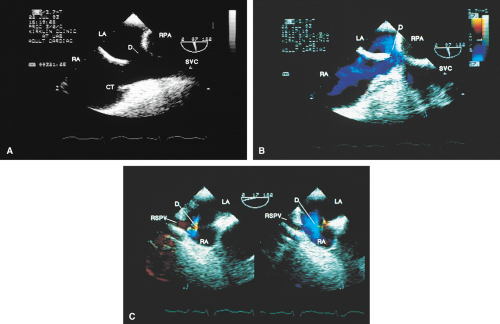 FIGURE 8.1.9. Sinus venosus atrial septal defect. A,B. Examination at a plane angulation of 97° demonstrates the defect (D) in the superior portion of the atrial septum. C. Color Doppler examination at a plane angulation of 17° shows the opening of the right superior pulmonary vein (RSPV) into the right atrium (RA). CT, crista terminalis; LA, left atrium; RPA, right pulmonary artery; SVC, superior vena cava. (Reproduced with permission from Maxted W, Finch A, Nanda NC, et al. Multiplane transesophgeal echocardiographic detection of sinus venosus atrial septal defect. Echocardiography 1995;12:139–143. ) |
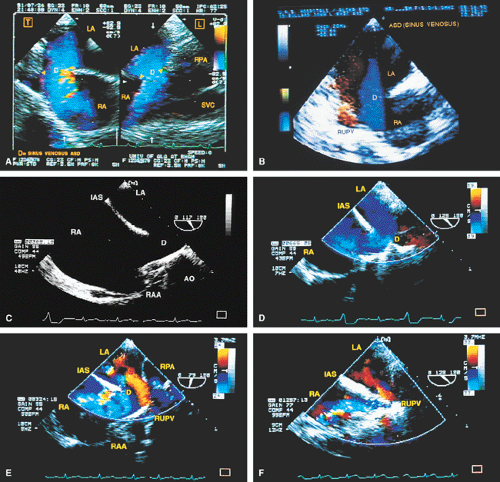 FIGURE 8.1.10. Sinus venosus atrial septal defect (ASD). A. A large defect (D) is seen in the transverse and longitudinal planes together with a left-to-right shunt. B. A large sinus venosus defect (D) with left-to-right shunting (blue signals) is shown in another patient. Flow signals (red) from an anomalous right upper pulmonary vein (RUPV) are seen moving into the right atrium (RA) and then through the defect into the left atrium (LA). C–F. Another patient with a large sinus venosus defect (D) with left-to-right shunting (D). E. Flow signals (red) are seen moving from an anomalous RUPV into RA and then through the defect into LA. F. Postoperative study shows patch closure of the defect. RUPV flow signals are now seen entering the LA. AO, aorta; IAS, atrial septum; RAA, right atrial appendage; RPA, right pulmonary artery; SVC, superior vena cava. |
 FIGURE 8.1.11. Isolated anomalous left upper pulmonary vein (LUPV) drainage. A. The left upper pulmonary vein (LPV) is imaged in its usual position. B. Instead of draining into the left atrium (LA), the LPV opens into the right atrium (RA) underneath the atrial septum (arrow). C. Estimation of shunt flow volume in isolated partial anomalous pulmonary venous connection in another patient. The Doppler spectral trace (right) was obtained by placing the pulsed Doppler sample volume cursor parallel to the flow direction in a pulmonary vein (left; APV), located on the left side but not connected to the LA. The shunt flow volume (L/min) was calculated as a product of the cross-sectional area of the anomalous pulmonary vein (APV) (obtained by the formula π D2/4, with D equal to 0.98 cm, representing the lumen width at the site of pulsed Doppler interrogation), the mean flow velocity (38 cm/sec), the flow duration (T, 0.79 sec), and the heart rate (84 beats/min), and dividing it by 1000. The shunt flow volume was calculated to be 1.90 L/min in this patient. RV, right ventricle. (C reproduced with permission from Mehta RH, Jain SP, Nanda NC, et al. Isolated partial anomalous pulmonary venous connection: echocardiographic diagnosis and a new color Doppler method to assess shunt volume. Am Heart J 1991;122:870–873. ) |
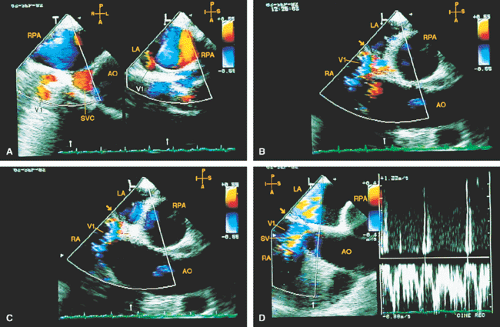 FIGURE 8.1.12. Isolated right-sided anomalous pulmonary venous return into the right atrium (RA). A. Simultaneous biplane (T, transverse plane; L, longitudinal plane) study shows red flow signals (V1) in the area normally occupied by the right superior pulmonary vein. Note that these flow signals do not extend into the left atrium (LA) as they normally should. B–D. Longitudinal plane examination. Prominent blue signals are noted in the RA in the vicinity of the right pulmonary artery (RPA) and originating just anterior to the interatrial septum (arrow), just across from where the right superior pulmonary vein signals should normally be seen entering the LA. These represent the RA entrance and the course of the flow signals from the anomalous pulmonary vein (V1). D. Spatial waveform obtained by pulsed Doppler interrogation of V1. AO, aorta; SV, sample volume; SVC, superior vena cava. (Reproduced with permission from Sanyal RS, Nanda NC, Snell D, et al. Transesophageal echocardiographic findings of complete unilateral anomalous pulmonary venous connection of right lung to right atrium. Echocardiography 1994;11:93–100. ) |
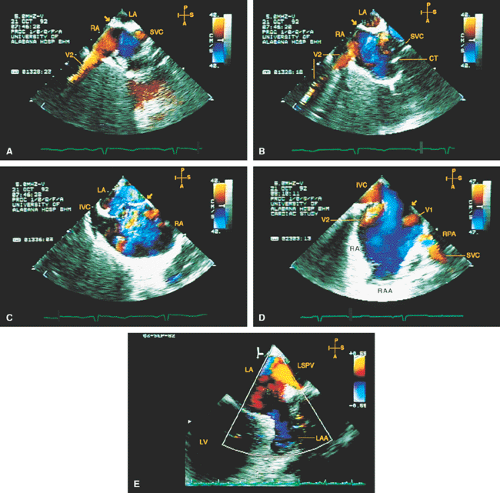 FIGURE 8.1.13. Isolated right-sided anomalous pulmonary venous return into the right atrium (RA). Same patient as in Figure 8.1.11. A–D. Longitudinal planes. A,B. The extracardiac course and the entrance of the second anomalous pulmonary vein (V2) into the RA are seen. C,D. The inferior vena cava (IVC) is separately visualized and enters the RA more posteriorly. E. The left superior pulmonary vein (LSPV) enters the left atrium (LA) normally. CT, crista terminalis; RAA, right atrial appendage; RPA, right pulmonary artery; SVC, superior vena cava. (Reproduced with permission from Sanyal RS, Nanda NC, Snell D, et al. Transesophageal echocardiographic findings of complete unilateral anomalous pulmonary venous connection of right lung to right atrium. Echocardiography 1994;11:93–100. ) |
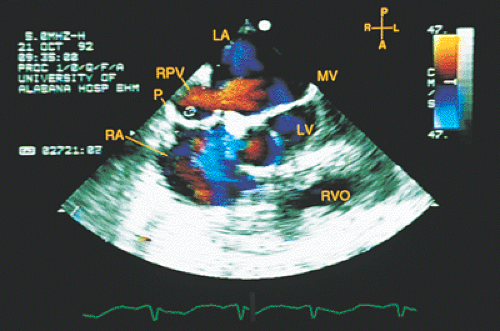 FIGURE 8.1.14. Isolated right-sided anomalous venous return into right atrium (RA). Same patient as in Figures 8.1.11 and 8.1.12. Transverse plane. Following surgery, pulmonary vein flow signals from the right side (RPV) are seen entering the left atrium (LA) posterior to the surgically inserted patch (P). LV, left ventricle; MV, mitral valve; RVO, right ventricular outflow tract. (Reproduced with permission from Sanyal RS, Nanda NC, Snell D, et al. Transesophageal echocardiographic findings of complete unilateral anomalous pulmonary venous connection of right lung to right atrium. Echocardiography 1994;11:93–100. ) |
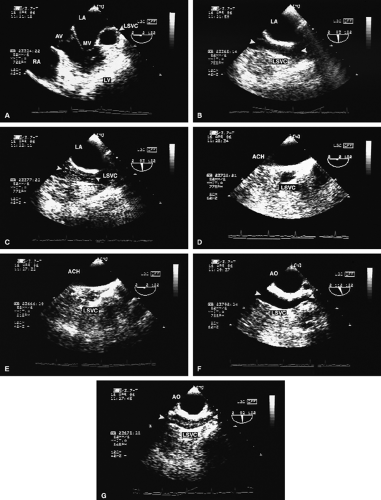 FIGURE 8.1.15. Left-sided superior vena cava (SVC). A–F. The large rounded echo-free space lateral to the MV in A is the left-sided superior vena cava (LSVC). Longitudinal plane examination (B,C) demonstrates the LSVC imaged anterior to the left atrium (LA). (B). C. Following intravenous left arm injection of normal saline, contrast signals are seen in the LSVC. D–G. The LSVC imaged behind the aortic arch (ACH) in the same patient. E–G. Contrast signals (arrowheads) in the LSVC following intravenous left arm injection of normal saline. In suspected cases, contrast echocardiography is useful in confirming the diagnosis. AO, aorta; AV, aortic valve; LV, left ventricle; MV, mitral valve; RV, right ventricle. |
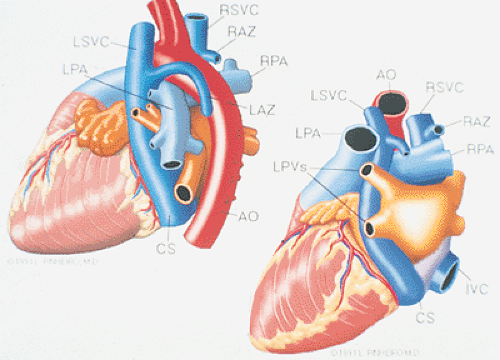 FIGURE 8.1.16. Left-sided superior vena cava (SVC). Diagrammatic representation of left-sided superior vena cava (LSVC) draining into the coronary sinus (CS). Left: the more common course of the LSVC, anterior to the left pulmonary artery (LPA). Right: the much less common course of LSVC, posterior to the LPA. AO, aorta; IVC, inferior vena cava; LAZ, left azygos vein; LPV, left-sided pulmonary veins; RAZ, right azygos vein; RSVC, right-sided superior vena cava. (Reproduced with permission from Nanda NC, Pinheiro L, Sanyal R, et al. Transesophageal echocardiographic examination of left-sided superior vena cava and azygos and hemiazygos veins. Echocardiography 1991;8:731–740. ) |
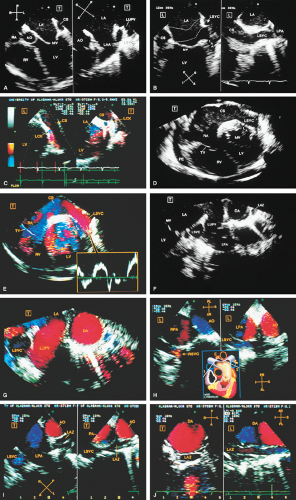 FIGURE 8.1.17. Left-sided superior vena cava (SVC) draining into the coronary sinus. A 47-year-old man with nephrotic syndrome and no other congenital cardiac abnormality. A. Transverse (T) imaging planes. The five-chamber (left) view shows enlargement of the coronary sinus (CS), resulting from drainage of the left-sided superior vena cava (LSVC), which is imaged in the aortic short-axis plane (right). B. Longitudinal (L) imaging planes. The two-chamber plane (left) views both the LSVC and the CS, but fails to show their continuity. Counterclockwise rotation of the transducer from this position shifts the plane to the left, resulting in a long-axis delineation of the LSVC and its entrance into the CS (right). C. The relationship of enlarged CS to left circumflex coronary artery (LCX) viewed in transverse and longitudinal planes. D,E. Composite illustrations shows the connection of the LSVC to the CS and their relationship to adjacent cardiac structures. The images used to generate each of these composites were taken from three different but adjacent transverse planes obtained by rotation with slight withdrawal of the probe when imaging the LSVC. E, inset. A spectral trace obtained from color Doppler–guided pulsed Doppler examination of the LSVC. F,G. Another set of composite illustrations, each acquired by combining two adjacent transverse plane images. These demonstrate the LSVC and left azygos vein (LAZ) and their relation to other cardiac structures. H. Longitudinal plane examination shows the relationship of the right SVC to the right pulmonary artery (RPA, left) and the relationship of the LSVC to the left pulmonary artery (LPA, right). The right-sided superior vena cava (RSVC) was imaged by clockwise rotation of the transducer so that the plane was shifted to the right (1 in the inset), whereas the LSVC was imaged by counterclockwise rotation, which moved the plane to the left (2 in the inset). I. Transverse plane examination demonstrates the LSVC located anterior to the LPA (left). The image on the right, obtained by slightly withdrawing the transducer, shows the entrance of the LAZ into the LSVC. Because the LAZ enters the LSVC in almost a perpendicular manner, the axes of the vessels are practically at right angles to each other. In this instance, the LAZ is imaged in long axis, whereas the LSVC is viewed in short axis. These images were obtained by withdrawing the transducer to acquire a standard transesophageal plane, which views the distal ascending aorta (DA) in short axis together with the main pulmonary artery bifurcation and then rotating the transducer counterclockwise to move the plane to the left. J. Transverse and longitudinal plane examination demonstrates the relation of the LAZ to the DA. These planes were obtained by advancing the transducer and rotating it counterclockwise (plane moves to the left) from the position used to obtain images shown in I. AO, aorta; LA, left atrium; LAA, left atrial appendage; LV, left ventricle; PE, pericardial effusion; RA, right atrium; RV, right ventricle. (Reproduced with permission from Nanda NC, Pinheiro L, Sanyal R, et al. Transesophageal echocardiographic examination of left-sided superior vena cava and azygos and hemiazygos veins. Echocardiography 1991;8:731–740. ) |
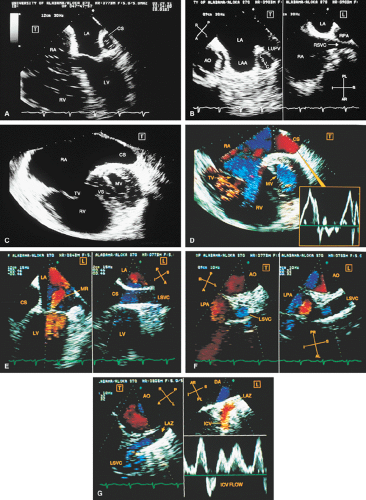 FIGURE 8.1.18. Left-sided superior vena cava (LSVC) draining into the coronary sinus. A 40-year-old woman, status postrepair of an atrial septal defect, presented with systemic hypertension, left ventricular hypertrophy, and mitral regurgitation (MR). A. Four-chamber view shows a dilated coronary sinus (CS) resulting from the drainage of the LSVC, noted at surgery for repair of atrial septal defect. Contrast injection into a left arm vein using normal saline demonstrates contrast echoes in the CS, right atrium (RA), and right ventricle (RV). B. Transverse plane examination (left) at the level of the aortic root (AO) demonstrates the relationship of the LSVC to the left atrial appendage (LAA) and left upper pulmonary vein (LUPV). Longitudinal plane examination (right) demonstrates the coexistence of a right-sided superior vena cava (RSVC). C,D. Composite illustrations prepared by combining two transverse plane images obtained by rotation of the transesophageal probe demonstrate an enlarged CS entering the RA. The inset in D represents a spectral trace obtained by color Doppler—guided pulsed Doppler interrogation of the CS. E. Longitudinal plane examination. The two-chamber view (left) shows marked enlargement of the CS. Note also the presence of MR in this systolic frame. Withdrawing the probe and rotating it counterclockwise (to shift the plane to the left) brings into view the entrance of the LSVC into the CS (right). F. The probe is withdrawn further to the level where the distal ascending aorta (DA) and the main pulmonary artery bifurcation are visualized. When the probe is rotated counterclockwise (to move the plane to the left), it demonstrates the LSVC (imaged in short axis) to be located posterior to the left pulmonary artery (LPA) and in the vicinity of the aorta (AO) in this transverse plane examination (left), in contrast to Figure 8.1.11, where the LSVC was located anterior to the LPA. In the longitudinal plane examination (right), the LSVC is imaged in long axis. G. Withdrawing the probe and rotating it counterclockwise to image the proximal DA brings into view the LAZ, which is seen to enter LSVC in the transverse plane examination (left). Longitudinal plane examination (right, top) shows a posterior intercostal vein (ICV) joining the LAZ posterior to the DA, viewed in long axis. The spectral trace (right, bottom) was obtained by color Doppler—guided pulsed Doppler interrogation of the ICV. LA, left atrium; LAZ, left azygos vein; LV, left ventricle; MV, mitral valve; RPA, right pulmonary artery; TV, tricuspid valve; VS, ventricular septum. (Reproduced with permission from Nanda NC, Pinheiro L, Sanyal R, et al. Transesophageal echocardiographic examination of left-sided superior vena cava and azygos and hemiazygos veins. Echocardiography 1991;8:731–740. ) |
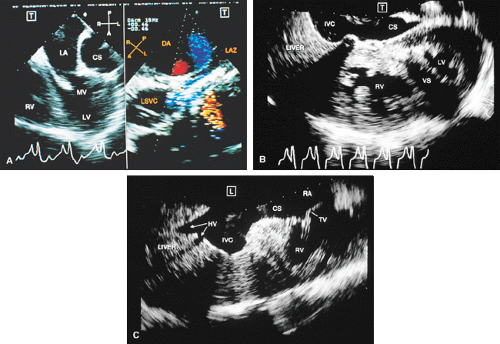 FIGURE 8.1.19. Left-sided superior vena cava (LSVC) entering the coronary sinus. A 20-year-old man with tetralogy of Fallot and pulmonary atresia. In this patient, the inferior vena cava (IVC) also drained into the coronary sinus (CS). The right superior vena cava (RSVC) drained normally into the right atrium (RA). A. Transverse plane examination shows enlargement of the CS due to LSVC drainage (left). Longitudinal plane examination (right) shows the left azygos vein (LAZ) joining the LSVC. B,C. Composite illustrations, each prepared by placing together contiguous images obtained during transverse (B) and longitudinal (C) plane examinations. The IVC is clearly seen entering the CS. This finding and the presence of LSVC were confirmed angiographically. DA, descending thoracic aorta; HV, hepatic vein; LA, left atrium; LV, left ventricle; MV, mitral valve; RV, right ventricle; TV, tricuspid valve; VS, ventricular septum. (Reproduced with permission from Nanda NC, Pinheiro L, Sanyal R, et al. Transesophageal echocardiographic examination of left-sided superior vena cava and azygos and hemiazygos veins. Echocardiography 1991;8:731–740. ) |
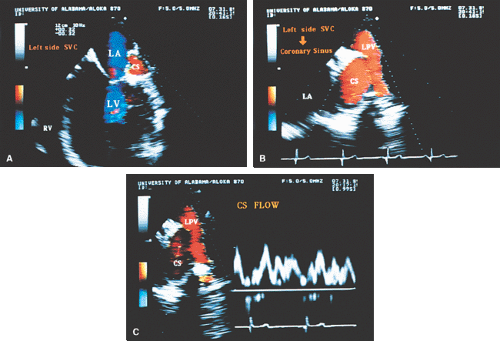 FIGURE 8.1.20. Left-sided superior vena cava (LSVC). A,B. Enlargement of the coronary sinus (CS) resulting from anomalous drainage of the left-sided superior vena cava (SVC). C. Pulsed Doppler interrogation of the enlarged coronary sinus shows prominent flow signals throughout the cardiac cycle. LA, left atrium; LPV, left upper pulmonary vein; LV, left ventricle; RV, right ventricle. |
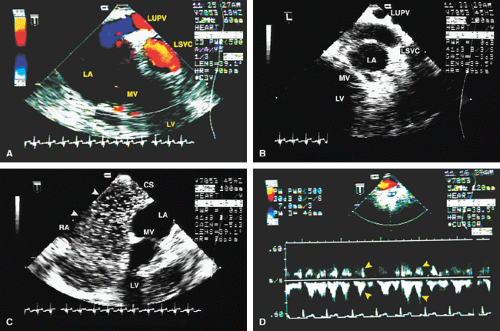 FIGURE 8.1.21. Left-sided superior vena cava (LSVC). A,B. Relationship of the LSVC to the left upper pulmonary vein (LUPV) and left atrium (LA). C. Contrast signals (arrowheads) moving from the markedly enlarged coronary sinus (CS) into the right atrium (RA) following a left arm vein saline contrast injection. The coronary sinus is enlarged as a result of the increased (anomalous) flow. D. Pulsed Doppler interrogation of the LSVC imaged behind the aorta in the same patient shows continuous flow throughout the cardiac cycle (arrowheads). LV, left ventricle; MV, mitral valve. |
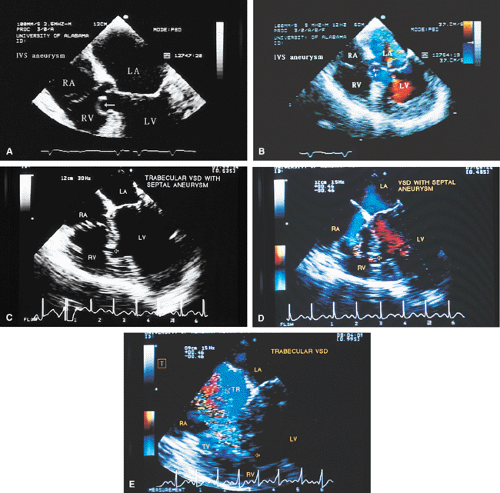 FIGURE 8.1.22. Ventricular septal aneurysm. A,B. An aneurysm (arrows) of the membranous septum bulging into the right ventricle (RV). C,D. Another patient with a trabecular ventricular septal aneurysm (arrows) associated with a defect. Flow signals are seen moving from left ventricle (LV) to the RV through the ventricular septal defect. E. Associated severe TR. IVS, ventricular septum; LA, left atrium; RA, right atrium; TV, tricuspid valve. |
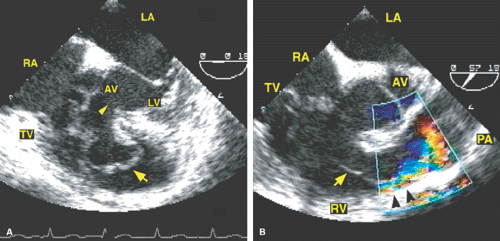 FIGURE 8.1.23. Transesophageal echocardiographic delineation of ventricular septal aneurysm producing right ventricular outflow obstruction in an adult. A. The arrow points to the ventricular septal aneurysm bulging into right ventricular outflow tract. The ventricular septal defect is delineated by the arrowhead. B. Color Doppler examination shows a narrow turbulent jet (black arrowheads) indicative of significant obstruction produced by the aneurysm (arrow). AV, aortic valve; LA, left atrium; LV, left ventricle; PA, pulmonary artery; RA, right atrium; RV, right ventricle; TV, tricuspid valve. (Reproduced with permission from Baweja G, Nanda NC, Nekkanti R, et al. Three-dimensional transesophageal echocardiographic delineation of ventricular septal aneurysm producing right ventricular outflow obstruction in an adult. Echocardiography 2004;21:95–97. ) |
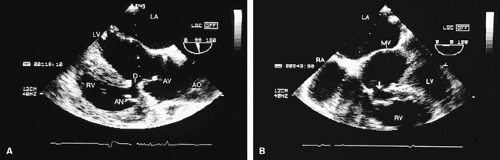 FIGURE 8.1.24. Perimembranous ventricular septal defect. The defect (D in A and the arrow in B) is demonstrated together with an aneurysm (AN) of the ventricular septum. AO, aorta; AV, aortic valve; LA, left atrium; LV, left ventricle; RV, right ventricle. |
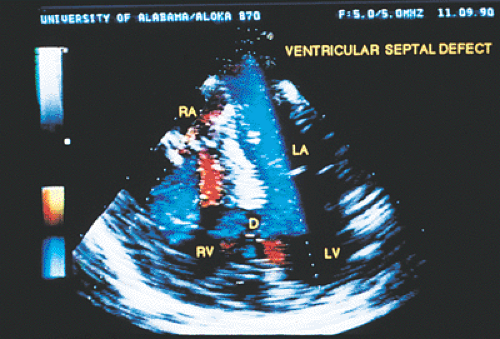 FIGURE 8.1.25. Trabecular ventricular septal defect. A large defect (D) is seen in the trabecular (muscular) portion of the ventricular septum (VS). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle. |
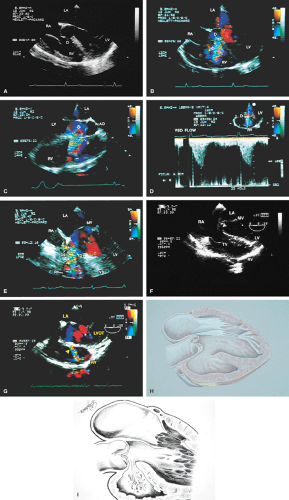 FIGURE 8.1.26. Perimembranous ventricular septal defect. A–E. A. A large defect (D) is seen just below the tricuspid valve (TV) and aortic valve with flow signals (arrow in B) moving through it into the right ventricle (RV). C. A large zone of flow acceleration (arrow) on the left ventricle (LV) side of the defect. Color Doppler–guided continuous wave Doppler shows a high velocity of 5 m/sec. Using the Bernoulli equation, this translates into a pressure gradient of 100 mm Hg across the defect. Because this patient’s systolic blood pressure was 125 mm Hg, the PA systolic pressure is estimated to be about 25 mm Hg. Thus, pulmonary hypertension is absent. E. A smaller second ventricular septal defect (VSD) (D2) is noted in addition to the large defect (D1) seen earlier. F,G. A perimembranous ventricular septal defect (arrowheads) with left-to-right shunting in another patient. H,I. Schematics show a perimembranous VSD. AO, aorta; LA, left atrium; LVOT, left ventricular outflow tract; MV, mitral valve; RA, right atrium; VS, ventricular septum. |
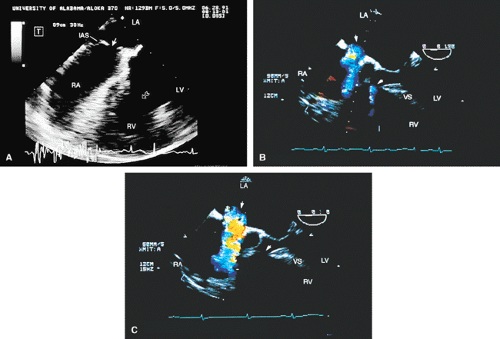 FIGURE 8.1.27. Ventricular septal (VS) defect associated with atrial septal (IAS) defect. A. A large ventricular septal defect (open arrow) and an associated secundum atrial septal defect (closed arrow). B,C. Color Doppler examination. B. Flow signals moving from the left atrium (LA) to the right atrium (RA) (upper arrow) and from the left ventricle (LV) to the right ventricle (RV) (lower arrow). C. The ventricular septal defect is seen just underneath the tricuspid valve (TV), demonstrating its perimembranous location. |
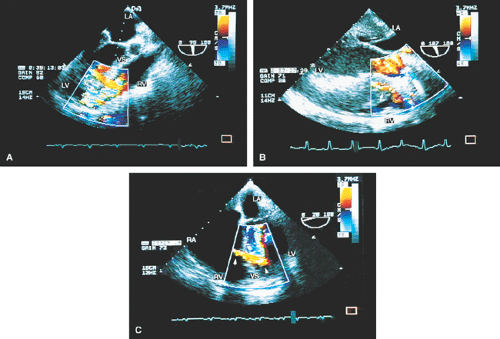 FIGURE 8.1.28. Ventricular septal defect mimic. A side-lobe artifact (arrows), which simulates the presence of a ventricular septal defect in all three patients shown here. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; VS, ventricular septum. |
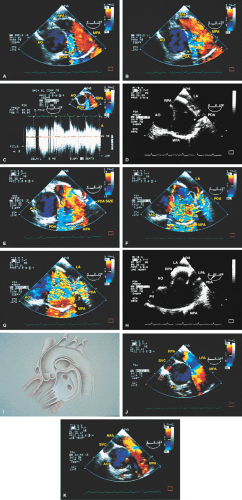 FIGURE 8.1.29. Patent ductus arteriosus. A,B. Turbulent flow (arrow) in the main pulmonary artery (MPA) produced by a patent ductus arteriosus (PDA) in this adult patient. C. Continuous wave Doppler examination shows flow throughout the cardiac cycle. D. The connection (arrow) between the PDA and the MPA. E–G. Color Doppler examination also delineates the PDA and its connection with the MPA. H. The relationship of the PDA with the MPA and the left pulmonary artery (LPA) is shown. I. Schematic shows a PDA. J,K. These views, obtained after surgery, show absence of turbulence in the MPA. AO, aorta; LA, left atrium; PV, pulmonary valve; RPA, right pulmonary artery; SVC, superior vena cava. |
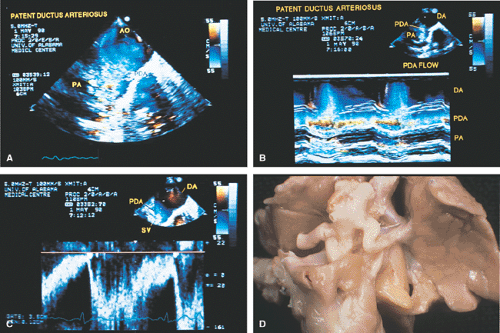 FIGURE 8.1.30. Patent ductus arteriosus (PDA). A. Color Doppler examination shows turbulent flow signals moving from the aorta (AO) into the pulmonary artery (PA) through the PDA. Color M-mode in B and pulsed Doppler in C show continuous flow throughout the cardiac cycle through the PDA. DA, descending aorta; SV, Doppler sample volume. D. Gross specimen shows a PDA. |
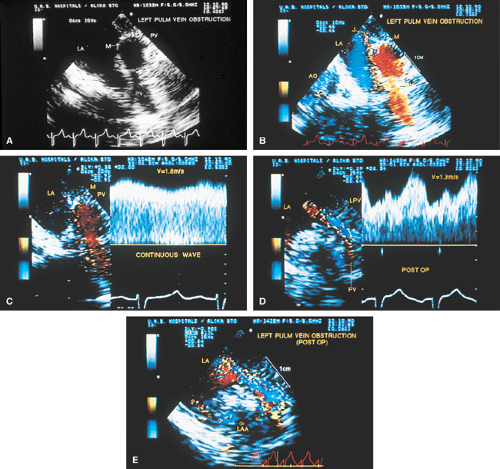 FIGURE 8.1.31. Left pulmonary vein (LPV) obstruction. A. An extensive, thick linear echo indicative of a membrane (M) is seen interposed between dilated left-sided pulmonary veins (PV) and the left atrium (LA) in this 9-year-old boy. B. Color Doppler examination. A narrow jet (J) is visualized originating from a small area of discontinuity in the membrane and moving into the LA. The jet measured 2 mm at its origin, indicative of severe obstruction. C. High-pulse-repetition-frequency Doppler interrogation of the jet demonstrates a high peak velocity of 1.8 m/sec and continuous flow throughout the cardiac cycle with little phasic variation. Note also the presence of spectral broadening, indicative of turbulent flow. D. Postoperative study. After surgical repair there is marked increase in proximal jet width to 7 mm; significant reduction in peak velocity to 1.3 m/sec; and development of prominent phasic variations. Spectral broadening is still noted and indicates persistence of turbulent flow. E. Postoperative study shows pulmonary veins communicating with the LA through two relatively wide channels, one located posteriorly (upper closed arrows) in the usual location of the pulmonary vein—the LA junction, and the other more anteriorly (lower closed and open arrows), representing direct anastomosis of the left common pulmonary vein with the left atrial appendage (LAA). AO, aorta. (Reproduced with permission from Samdarshi TE, Morrow R, Helmcke FR, et al. Assessment of pulmonary vein stenosis by transesophageal echocardiography. Am Heart J 1991;122:1495–1498. ) |
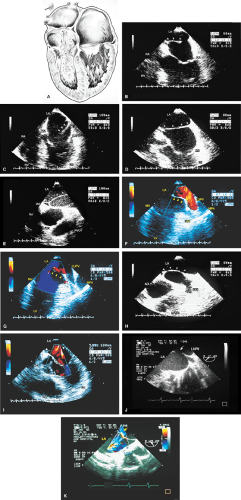 FIGURE 8.1.32. Cor triatriatum. A. The schematic shows a membrane separating the left atrium (LA) into two chambers, with pulmonary veins on one side and the left atrial appendage (LAA) on the other. Notice the small orifice in the membrane causing obstruction to blood flow. B–I. An adult patient with a cor triatriatum membrane (arrowheads). In F through H, the membrane appears to be an extension of the “Q-tip” separating the LAA from the left upper pulmonary vein (LUPV). In E, the membrane (arrowheads) appears to have a double attachment to the interatrial septum (IAS). G,I. Color Doppler examination shows laminar flow signals moving through the membrane, indicating the absence of obstruction. J,K. Another adult patient with cor triatriatum. J. A wide opening (1.4 cm; arrow) in the membrane is seen separating the LUPV from the LAA. K. Color Doppler study demonstrates some turbulence, but the peak velocity measured less than 1 m/sec, indicating the absence of any significant obstruction to flow. AO, aorta; AV, aortic valve; IVS, ventricular septum; LV, left ventricle; MPA, main pulmonary artery; MV, mitral valve; RA, right atrium; RV, right ventricle. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


