31 Outcome of Fetal Congenital Heart Defects
I. INTRODUCTION
A. Rationale
1. The goal of prenatal diagnosis is the near-term delivery of a nonhydropic infant whose postnatal management is anticipated.
2. Fetuses with structural cardiac defects are at increased risk for heart failure, premature delivery, and fetal demise.
3. One quarter of all infant deaths are due to congenital anomalies, and one third of these are cardiac defects.
4. In utero interventions for structural defects are not without risk, and data suggesting that intervention substantially alters the natural history are limited. In this chapter we review the outcome of fetuses presenting with structural cardiac defects.
B. Prenatal examination
1. It is estimated that 80% of all pregnant women have at least one ultrasound during pregnancy.
2. Both the International Society of Ultrasound in Obstetrics and Gynecology and the American Institute of Ultrasound in Medicine recommend that assessment of the fetal heart in the structural survey include both the four-chamber and outflow-tract views.
a. The four-chamber view alone can detect at best 60% of congenital cardiac defects.
b. Incorporating views of the left and right outflow tracts can further increase the detection of cardiac defects to 85% to 90%, including ductus-dependent lesions.
c. Secular trends show an increasing number of infants presenting for surgery with in utero diagnoses.
II. OVERALL OUTCOME OF FETAL CONGENITAL HEART DEFECTS
A. Historical outcomes
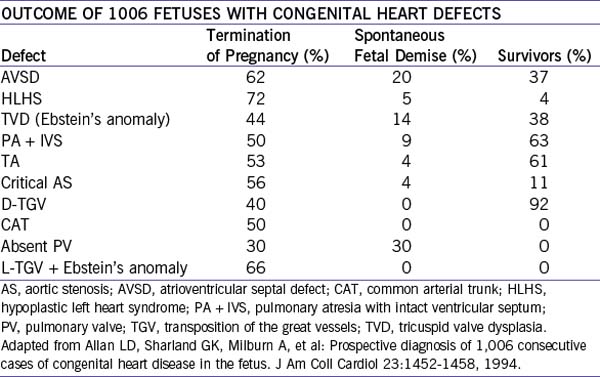
1. In Allen and colleagues’ (2005) series, the overall outcome of 1006 fetuses with diagnosed congenital heart defects (1980-1993) was fairly bleak, with a high percentage of interrupted pregnancies.
2. About 17% had associated chromosomal anomalies.
3. Survivors of continuing pregnancies ranged from 92% with D-transposition of the great vessels to 0% with common arterial trunk, tetralogy of Fallot with absent pulmonary valve, or L-transposition of the great vessels with Ebstein’s malformation of the tricuspid valve (Table 31-1).
B. Current outcomes
1. Outcomes of the fetus with prenatally diagnosed congenital heart disease have improved somewhat in more recent studies, with overall survival ranging from 45% to 60% in 93 to 408 cases.
2. Pregnancy interruptions decreased to 23% to 35% in these newer series.
3. Very few series have shown improved survival in infants with heart defects diagnosed before birth.
III. OUTCOME OF SPECIFIC HEART DEFECTS
A. Heterotaxy syndromes
1. The heterotaxy syndromes include right and left atrial isomerisms (RAI and LAI).
2. In general, mortality of RAI and LAI is high due to the complexity of the structural defects in both and to the high percentage of patients with complete atrioventricular block (AVB) in LAI.
a. Long-term survival with RAI is 13% to 40%.
b. Long-term survival for LAI is 14% to 52%.
4. Nonsurvival correlates with atrioventricular block and hydrops.
a. Many (33%-45%) of these pregnancies are interrupted or have intrauterine demise.
b. Prenatal diagnosis might confer no survival advantage for either LAI or RAI.
B. Common arterial trunk
1. There have been two small series, one of 17 and the other of 23 fetuses.
b. Overall survival was 35% or 42%. Integrity of the truncal valve influences long-term survival.
2. It is unknown if other factors frequent in common arterial trunk, such as the 22q11 deletion, branch pulmonary artery stenosis, and interrupted aortic arch, affect either prenatal or postnatal outcomes.



