22 Other Indications

Fig. 22.1
a Malignant pericardial effusion. View of the pericardium from the left side.
b Thoracoscopic pericardial fenestration. Same case, showing the fenestration of the pericardium created by laser coagulation.
(Courtesy of B. Vogel and W. Mall.)
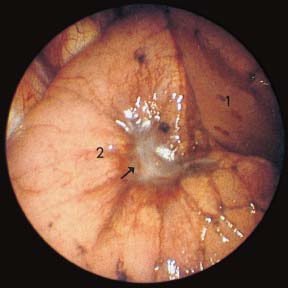
Fig. 22.2
Adenocarcinoma of the lung with malignant retraction. After induction of a right-sided pneumothorax, the upper lobe (1) is unremarkable. In the apex of the lower lobe (2) there is typical carcinomatous retraction (→) with radiating scars particularly on the interlobar fissure. In the center, covered with shiny pleura, the tumor is seen as a yellowish-gray mass.
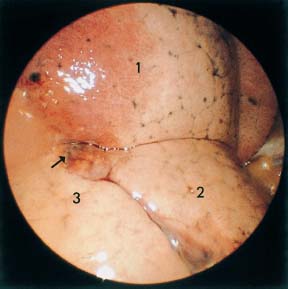
Fig. 22.3
Hamartochondroma. After iatrogenic pneumothorax due to fine-needle aspiration, the pneumothorax was utilized for thoracoscopy. The apex of the right lower lobe (1) is congested as a result of the needle aspiration; the laterobasal segment (2) is separated by the intersegmental septum. The posterobasal segment (3) shows, on its leading edge, an irregular gray-brown lesion (→) which is also somewhat hemorrhagic as a result of the previous puncture.
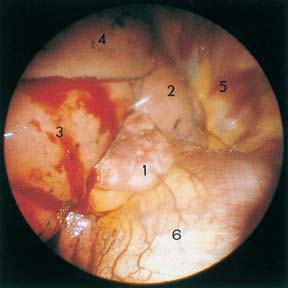
Fig. 22.4
Leiomyofibroma of the middle lobe. After iatrogenic right-sided pneumothorax due to transthoracic needle aspiration: a yellowish-gray irregular tumor, 2 cm × 3 cm (1), between the middle lobe (2) and lower lobe (3), covered with fresh blood. The upper lobe (4) is covered by delicate pleura, the anterior chest wall (5), and the diaphragm (6). Surgery revealed that the leiomyofibroma originated from the middle lobe.
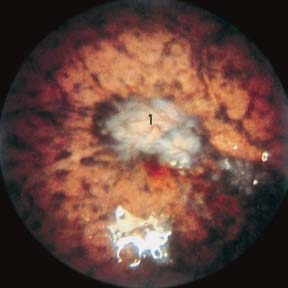
Fig. 22.5
Multiple bilateral tuberculomas. After induction of a right-sided pneumothorax, the lung shows spotty pigmentation. In several areas are whitish-gray foci extending to 1 cm diameter, infiltrated with vessels and with a pigmented border. Atypical focus (1) on the periphery of the upper lobe; histologically scarred tuberculoma with fresh epitheloid cell satellite lesions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


