1. How does warfarin work?
Warfarin (and related coumarin compounds) inhibit the activity of hepatic vitamin K-2,3 epoxide, which is used to recycle the active form of vitamin K, vitamin K hydroquinone. Without sufficient vitamin K hydroquinone, clotting factors II, VII, IX, and X fail to be carboxylated, leaving them in an inactive state. The onset of warfarin anticoagulation is gradual and related to the elimination half-lives of the already synthesized active forms of these procoagulation factors. In addition to inhibiting the formation of active factors II, VII, IX, and X, warfarin also inhibits the vitamin K–dependent formation of two coagulation inhibitors, proteins C and S, which may temporarily create a relative procoagulant state until full anticoagulation is achieved. Warfarin is a racemic mixture of S and R isomers. The S isomer has more inhibitory activity and is metabolized primarily by cytochrome P-450 (CYP) isoform 2C9 (CYP2C9), which is the major source of drug interactions with warfarin. The R isomer is metabolized primarily by CYP3A4 and CYP1A2, resulting in additional drug interactions.
2. What are the clinical situations in which warfarin is used and at what anticoagulation intensity?
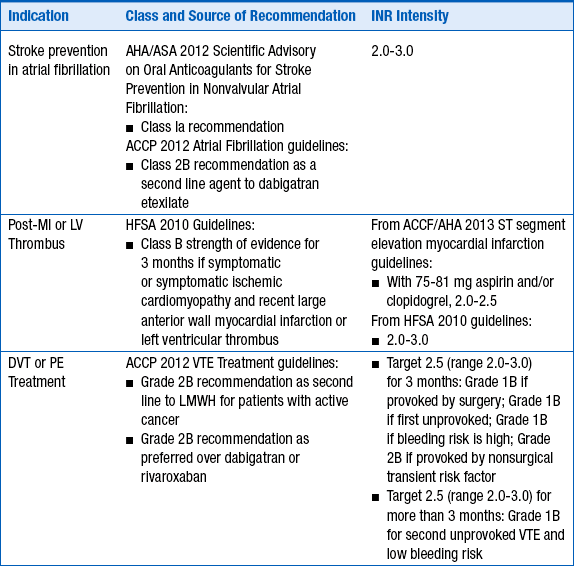
The intensity of anticoagulation with warfarin depends primarily on the indication for anticoagulation. These are given in Table 53-1 .
TABLE 53-1
INDICATIONS FOR ANTICOAGULATION WITH WARFARIN AND RECOMMENDED INTERNATIONAL NORMALIZED RATIO INTENSITY
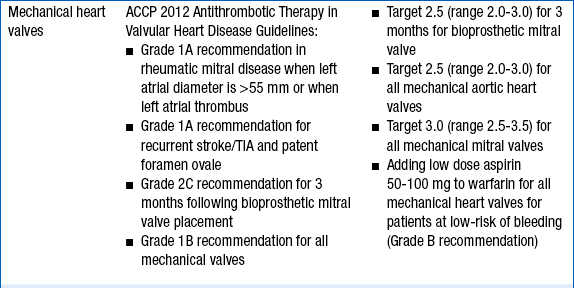
ACCF , American College of Cardiology Foundation; ACCP , American College of Chest Physicians; AHA , American Heart Association; ASA , American Stroke Association; DVT , deep vein thrombosis; ESC , European Society of Cardiology; HFSA , Heart Failure Society of America; INR , international normalized ratio; LV , left ventricular; MI , myocardial infarction; PE , pulmonary embolism; TIA , transient ischemic attack; VTE , venous thromboembolism.
3. What is the role of warfarin in preventing transient ischemic attack and stroke in a patient with a history of ischemic stroke?
For most patients with noncardioembolic ischemic stroke, the underlying pathophysiology is similar to that of acute coronary syndromes—that is, arterial atherothrombosis. Therefore, antiplatelet drugs, either alone or in combination, have been slightly superior to warfarin in comparative trials for stroke prevention. In addition, despite no clinical advantage, the warfarin patients experience much more major and minor bleeding. Thus, warfarin has no role in the treatment of ischemic stroke (class Ia recommendation from American College of Chest Physicians [ACCP] 2012 guidelines for antiplatelet therapy rather than oral anticoagulation).
4. How should unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), or fondaparinux be overlapped with warfarin for acute treatment of venous thromboembolism?
Regardless of the parenteral agent chosen for initial anticoagulation, warfarin should be initiated on day 1 of treatment. Choice of dose must be individualized based on patient-specific factors (age, concurrent medications, nutrition status, and comorbidities). However, for most patients, 5 mg daily is an adequate starting dose. According to the ACCP’s Antithrombotic Therapy and Prevention of Thrombosis, 9th edition, for younger, “healthier” patients, consideration may be given for initiating warfarin at 10 mg daily. UFH, LMWH, or fondaparinux should be overlapped with warfarin for a minimum of 4 to 5 days and until the international normalized ratio (INR) is therapeutic (INR more than 2.5 for 1 day, or more than 2.0 for 2 consecutive days). Recommended procedures for switching between warfarin and the newer oral anticoagulants dabigatran etexilate, apixaban, and rivaroxaban are reviewed in Question 14.
5. What is the role of pharmacogenomics in warfarin dosing?
Warfarin dosing is challenging, in part, because of the varied response and the wide range of doses required to achieve a therapeutic INR in an individual patient. Contributors to this variability are polymorphisms in the CYP2C9 metabolizing enzyme responsible for the majority of warfarin metabolism, and in the target enzyme for warfarin, vitamin K epoxide reductase. Patients with either or both of these genetic polymorphisms tend to be more sensitive to warfarin and require lower doses. As genetic testing for these polymorphisms becomes less expensive and more accessible, pharmacogenetic dose selection may allow for a shorter time to a therapeutic INR and reduced bleeding complications. For these reasons, the 2012 ACCP Guidelines recommend against pharmacogenetic testing for patients initiating warfarin at this time.
6. How should warfarin be managed in patients who need surgery?
For patients who need INR normalized before surgery, warfarin should be stopped 5 days before the surgery. Depending on the reason for anticoagulation, bridging may be necessary. The most common indications for bridging therapy are patients with mechanical valves and recent deep vein thrombosis (DVT) and/or pulmonary embolism (PE). These patients should receive full-dose subcutaneous (subcut) LMWH during the bridging period. The last dose of LMWH should be given no later than 24 hours before the procedure. LMWH should be resumed 24 to 48 hours (the next evening) after the procedure, depending on bleeding and thrombotic risks of the patient. Warfarin should be restarted within 12 to 24 hours after (evening of or next morning) of the procedure with risk somewhat mitigated by delayed onset of effect. The reader should be aware that, as with many drugs, although LMWH is not approved for bridging, it is often used for this purpose. Different practitioners will have different thresholds of confidence for the use of LMWH as a bridging agent. The most caution in exercising decisions regarding outpatient LMWH bridging versus inpatient intravenous UFH bridging should be in patients with mechanical mitral valves (as the low pressure gradient between the left atrium and left ventricle during diastole may increase the risks of thrombosis compared with mechanical valves in the aortic position). A 2008 Guideline from the American College of Cardiology Foundation (ACCF) and American Heart Association (AHA) discusses bridging and the role of LMWH (see Suggested Readings).
For patients who need urgent surgery, it is recommended to give intravenous vitamin K, 5 to 10 mg. Fresh frozen plasma or other similar agents will give a more rapid (albeit temporary) reversal of anticoagulation therapy and can be combined with vitamin K. For patients with warfarin-associated major bleeding, prothrombin complex concentrates, rather than plasma are recommended for reversal, in combination with intravenous vitamin K.
Relatively minor surgeries, such as dental and dermatologic procedures, do not generally require the discontinuation of warfarin. Typically, any excess in bleeding related to those procedures can be managed with local hemostatic agents.
7. What are some of the common drug interactions with warfarin?
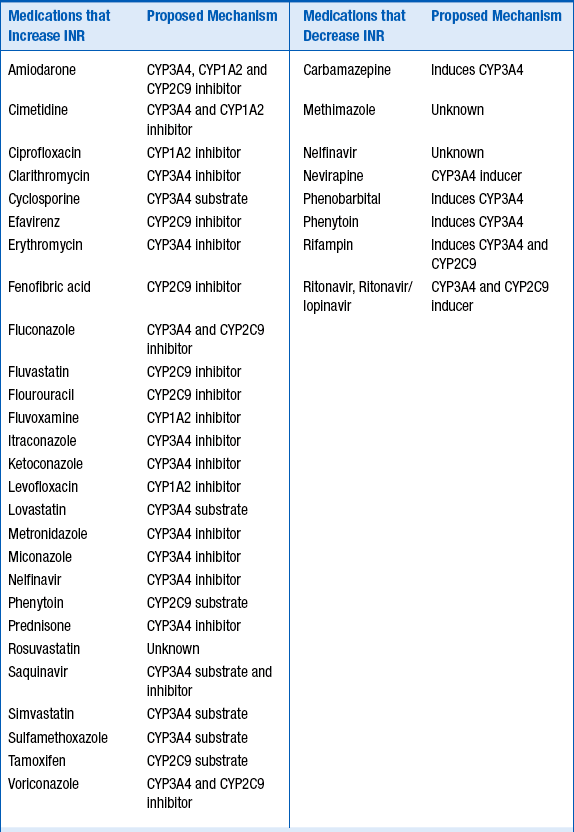
Because of its complex metabolism and relatively narrow therapeutic index, drug interactions involving warfarin are both common and clinically significant. The majority of the interactions occur at the level of CYP metabolism, although other mechanisms may be possible. Table 53-2 lists some of the more common interactions.
For the medications listed in Table 53-2 , the strength of the clinical evidence is sufficient to expect a change in INR, requiring either adjusting the warfarin dose up or down by 25% to 50% in anticipation of the resulting change in INR, or frequent INR monitoring to determine the dose adjustment necessary.
Foods and supplements may also alter the INR. Foods that increase the INR include garlic, mango, ginseng, grapefruit juice, and possibly cranberry juice. Ginger and fish oil have additive antithrombotic effects. Foods and supplements that reduce the INR include high vitamin K–content foods, enteral feeds, and soy milk.
8. How should warfarin be managed in patients with underlying chronic liver disease?
Management of warfarin in patients with underlying significant liver disease can be difficult. In addition to elevated baseline INRs, these patients often have low protein stores, thrombocytopenia, and reduced hepatic clearance, making them especially sensitive to effects of warfarin and more likely to have significant bleeding issues. Recommendations include lower starting doses and more frequent laboratory and clinical monitoring.
9. How should elevated INRs in patients taking warfarin be managed?
If there is no overt evidence of bleeding and rapid reversal is not necessary, the 2012 ACCP guidelines recommend against routine vitamin K administration unless the INR is more than 10. For INRs less than 4.5 without bleeding, the guidelines recommend lowering the dose or holding the next dose with frequent INR monitoring until the INR is within the therapeutic range and then resuming a lower dose. For INRs 4.5 to 10 without bleeding, the 2012 ACCP guidelines recommend omitting 1 to 2 doses, frequent INR monitoring, and resuming a lower warfarin dose when the INR is within the therapeutic range. When the INR is greater than 10 without overt bleeding, the 2012 ACCP guidelines recommend low-dose (5 mg or less) oral vitamin K.
For patients experiencing minor bleeding with an elevated INR, oral vitamin K is recommended at a dose of 2.5 to 5 mg, repeated at 24 hour intervals until the INR is within the therapeutic range and then resuming a lower dose of warfarin.
10. What are important patient counseling points for warfarin?
A patient medication guide is mandated to be dispensed by pharmacists to patients receiving prescriptions for warfarin. Important counseling points are:
Explain to patients the reason for warfarin therapy.
Explain the meaning and significance of the INR.
Identify each patient’s warfarin prescriber, current INR, and date of next scheduled INR test.
Explain the need for frequent INR testing and the target INR for each patient’s medical condition(s).
Explain the importance of compliance with therapy and related laboratory work (INR checks).
Describe common sites and signs of bleeding and what to do if they occur. Explain that bleeding and bruising are more likely to occur and that common sites of bleeding include the gums, urinary tract, and nose. Patients should be aware of any changes in stool color and to report dark, tarry stools to the health care provider immediately. Patients should also report any uncontrolled bleeding to the health care provider.
Counsel patients to avoid alcohol and activities or sports that may result in a fall or injury.
Explain how consuming foods containing vitamin K may impact the effectiveness of warfarin therapy and that the most important thing concerning the diet is not to make any significant changes without talking to the health care provider.
Explain to patients the importance of telling all health care providers that warfarin is being taken and that the health care provider prescribing warfarin needs to be informed of all scenarios where warfarin might need to be held (e.g., dental work, surgery, and other invasive procedures).
Explain to patients the importance of contacting the pharmacy if the color of the warfarin tablet is different.
Explain that warfarin should be taken at the same time each day and that if a dose is missed and it is within 12 hours of when the dose was supposed to be taken, it is okay to take the dose. Otherwise, the dose should be skipped and resumed the next day. The dose should not be doubled.
Discuss potential drug interactions. Explain that patients should contact their warfarin prescriber before taking any over-the-counter medications (including herbal supplements) or if a different health care provider starts them on a new medication (especially antibiotics).
Explain that women of child-bearing age must use birth control measures and notify their health care provider immediately if they become pregnant.
Advise patients to carry identification noting that they are taking warfarin.
Depending on the indication for warfarin, counsel patients on signs of clotting (e.g., calf pain, redness, swelling, shortness of breath, and stroke symptoms).
Document that the patient education session has occurred.
11. What are potential advantages of the newer oral anticoagulants dabigatran etexilate, apixaban, and rivaroxaban?
Only gold members can continue reading.
Log In or
Register to continue
Related
Stay updated, free articles. Join our Telegram channel
Join
Full access? Get Clinical Tree
 Explain to patients the reason for warfarin therapy.
Explain to patients the reason for warfarin therapy. Explain the meaning and significance of the INR.
Explain the meaning and significance of the INR. Identify each patient’s warfarin prescriber, current INR, and date of next scheduled INR test.
Identify each patient’s warfarin prescriber, current INR, and date of next scheduled INR test.
 Explain the importance of compliance with therapy and related laboratory work (INR checks).
Explain the importance of compliance with therapy and related laboratory work (INR checks).
 Counsel patients to avoid alcohol and activities or sports that may result in a fall or injury.
Counsel patients to avoid alcohol and activities or sports that may result in a fall or injury.





 Advise patients to carry identification noting that they are taking warfarin.
Advise patients to carry identification noting that they are taking warfarin.




