Chapter 34 Nutrition and Disorders of Gastrointestinal and Hepatic Function
Serious gastrointestinal complications are rare following cardiac surgery; the overall incidence is about 1%.1–3 However, when they do occur, they result in prolonged stays in the intensive care unit (ICU) and hospital, increased treatment costs, and high mortality rates. Early diagnosis is essential to prevent adverse outcomes but may be difficult in critically ill patients in whom the signs of intraabdominal disease are masked by sedation, mechanical ventilation, and cardiac disease. In patients with unexpected multiorgan dysfunction, an intraabdominal cause should always be suspected. Aggressive abdominal investigation and early consultation with a gastrointestinal surgeon are recommended because early laparoscopy or laparotomy may be lifesaving.
NUTRITION
Critically ill patients have increased metabolic rates and undergo accelerated protein catabolism. Fever, sepsis, catecholamines, trauma, and major surgery all increase energy expenditure, whereas hypothermia, inactivity, sedation, neuromuscular paralysis, and β-adrenergic blocking drugs reduce it. Under the influence of high levels of cortisol and catecholamines and of reduced insulin effect (see Chapter 2), there is increased release of amino acids from skeletal muscle. These amino acids are used largely as substrate for hepatic gluconeogenesis, with the nitrogen being released as urea and excreted by the kidneys. In highly catabolic patients, urinary nitrogen losses can exceed 30 g/day, which corresponds to about 200 g/day of protein mass. Although nutritional support does not prevent enhanced protein catabolism, it does reduce net protein loss; that is, feeding increases protein synthesis but does not prevent catabolism. After routine cardiac surgery that includes hypothermic cardiopulmonary bypass, nitrogen losses are usually modest and similar to those observed in the nonstressed fasting state.4
Nutrition Requirements
In some critically ill patients, energy expenditure is greatly increased. For instance, values in excess of 40 kcal/kg/day have been reported in patients with trauma and sepsis.5 By contrast, energy requirements are not typically significantly elevated following routine cardiac surgery6 and in other forms of critical illness.7 Furthermore, high energy nutrition (>30 to 35 kcal/kg/day), particularly when administered parenterally, can lead to metabolic complications.8 Excess carbohydrate administration can cause hyperglycemia, hyperlipidemia, and the accumulation of fat in the liver. Hyperglycemia exacerbates hypercarbic respiratory failure and is associated with an increased risk of postoperative infection, particularly of sternal wounds.9,10 Excess protein administration exacerbates azotemia and may precipitate uremic encephalopathy and coagulopathy. It can also cause hypertonic dehydration and metabolic acidosis, particularly when urine-concentrating ability is impaired. Excess fat administration can cause hyperlipidemia and may predispose to infection.
In an individual patient, energy requirements may be estimated using weight-based empirical formulas, such as the Harris-Benedict11 or Schofield equations,12 or they may be measured using indirect calorimetry, in which energy expenditure is calculated on the basis of measured oxygen consumption and carbon dioxide production. However, these calculations are not usually necessary; for most patients, initial administration of 25 kcal/kg/day (about 100 kJ/kg/day) is adequate.13,14 Indirect calorimetry to rule out overfeeding is useful in patients who are difficult to wean from mechanical ventilation. It should also be performed in patients who require prolonged nutritional support because 25 kcal/kg/day may be inadequate late in the clinical course.14 Indirect calorimetry is easily performed at the bedside.
Energy is provided as a combination of nitrogen compounds (amino acids, proteins), carbohydrates (glucose, oligosaccharides, polysaccharides), and fat (fatty acids, triglycerides). Administration of 1.2 to 1.5 g/kg/day of protein is recommended13; this corresponds to 0.2 to 0.24 g/kg/day of nitrogen, or 15% to 20% of total calories. Lower levels of nitrogen (e.g., 0.15 g/kg/day) should be administered in patients with renal dysfunction (not requiring renal replacement therapy) or hepatic dysfunction, and higher levels (0.3 g/kg/day) may be given to severely catabolic patients. Fat should constitute about 20% to 30% of calories, with the remaining provided as carbohydrate.13 Fat should not exceed 2.5 g/kg/day and carbohydrate should not exceed 6 g/kg/day. Energy density is greatest with fat (~9 kcal/g) compared with carbohydrate and protein, which are both about 4 kcal/g. Nutritional support should also contain micronutrients: vitamins, minerals, and trace elements.15 Potassium, magnesium, and phosphate should be provided in sufficient quantities to maintain normal plasma levels.
Enteral Versus Parenteral Nutrition
Nutrition may be given enterally or parenterally. Enteral nutrition may be delivered into the stomach via a nasogastric tube or postpylorically into the small bowel via a nasojejunal tube. Enteral nutrition has the advantages of being simpler and cheaper than parenteral nutrition, and it is associated with fewer infectious complications in certain patient populations16–18 (although this has not been studied specifically in cardiac surgery patients). The reduction in infectious complications may be the result of the immunosuppressive effects of parenteral nutrition or because enteral nutrition may protect against the translocation of gastrointestinal microorganisms into the systemic circulation. Enteral nutrition also results in improved tolerance of carbohydrates compared with parenteral nutrition, with a reduced likelihood of developing hyperglycemia and its attendant complications.
Some clinicians consider enteral nutrition to be contraindicated in patients with severe circulatory compromise because of the potential for developing splanchnic oxygen supply-demand mismatch, in which the increased metabolic requirements of gut cannot be met by increased blood flow—a situation that could potentially cause mesenteric ischemia. However, in practice, this concern does not appear to be justified.19 Although gastric stasis is common, postpyloric delivery of enteral nutrition results in splanchnic vasodilation and nutrient absorption, even in postoperative cardiac patients with circulatory compromise.20–22 However, underfeeding is a possibility and caloric intake should be carefully monitored.22
Patients with persistent intolerance of enteral nutrition or gastrointestinal failure (e.g., due to small bowel ileus or mechanical obstruction) should receive parenteral nutrition. There may be a survival benefit in critically ill patients for early parenteral nutrition over delayed enteral nutrition.17 Combined support with enteral and parenteral nutrition may be considered in patients who are unable to achieve nutritional goals by means of enteral nutrition alone.
Enteral Nutrition
Composition
Most commercially available enteral feeds have an energy content of 1 to 2 kcal/ml; a value of 1.0 to 1.2 kcal/ml is typical (Table 34-1). Thus, a 70-kg patient receiving 25 kcal/kg/day has an obligatory fluid load of 1 to 2 l/day. Nitrogen is administered as protein (e.g., a soy isolate), carbohydrate as polysaccharides (e.g., corn syrup or hydrolyzed corn starch), and fat as triglycerides (e.g., canola oil). Micronutrients are added in appropriate quantities. Fiber and electrolytes are present in variable amounts.
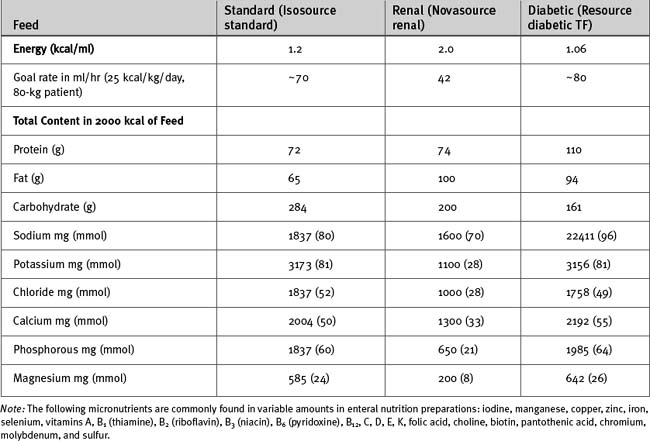
A wide variety of different enteral feeds are available for use in specific circumstances; only some of them are clinically useful. Elemental feeds, in which the nitrogen content is provided as amino acids, are useful in patients with short bowel syndrome, pancreatic insufficiency, and radiation enteritis, but they offer no advantage in the critically ill. Renal formulations that are calorie dense (typically 2 kcal/ml) and low in volume, sodium, and potassium are available. They are useful in patients with oliguric renal failure but should not be used in lieu of renal replacement therapy when it is indicated (see Chapter 33). Formulations for patients with diabetes, in which the carbohydrate content is reduced and the protein and fat content is increased, are available. However, the high protein content may be inappropriate for patients with renal dysfunction, and hyperglycemia is best managed by intravenous insulin rather than by carbohydrate restriction. Thus, diabetic formulations are infrequently used in the ICU. The use of so-called immune-enhancing feeds is controversial. Guidelines do not support the use of arginine-enriched feeds, but they offer limited support for the use of feeds supplemented by glutamine (for patients with burns and trauma) and by fish oils, borage oils, and antioxidants (for patients with acute respiratory distress syndrome).16 Formulations that are high in fat (50% of calories) and low in carbohydrate and sodium are available for use in patients with acute respiratory distress syndrome; they may have a role in selected patients who have hypercarbic respiratory failure.
Route of Administration and Feeding Protocols
Nasogastric Feeding.
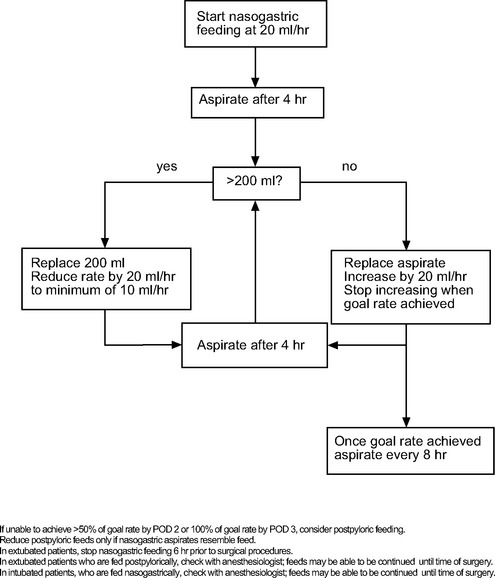
Consensus guidelines recommend starting enteral nutrition within 24 to 48 hours of ICU admission.16 Therefore, in all patients who are not expected to be extubated within 24 to 48 hours of surgery, a 12F or 14F nasogastric tube should be inserted on the first postoperative day. If the hemodynamic state permits, patients should be nursed at a 45-degree head-up position to help prevent aspiration of gastric contents and reduce the incidence of ventilator-associated pneumonia.23 Patients with intraaortic balloon pump in situ may be safely nursed at a 20-degree head-up position. Nasogastric feeding should be commenced at a low rate (e.g., 20 ml/hr). In critically ill patients who are receiving high doses of inotropic drugs, it may be prudent to maintain this low rate for the first 24 to 48 hours. Otherwise, the rate should be increased incrementally to the goal value according to protocol, an example of which is shown in Figure 34-1. The target rate should be determined on an individual basis. Aspirates in excess of 200 ml are indicative of gastric stasis. Metoclopramide (10 mg every 6 hours intravenously) may be used to promote gastric motility, but it is only weakly effective. Erythromycin is a more effective prokinetic than metoclopramide, but because it is potentially proarrhythmic and may promote antimicrobial resistance, its use for this purpose is not recommended.16
Nasojejunal Feeding.
If by postoperative day 3, gastric aspirates remain high and the target feeding rate has not been achieved, a fine-bore (10F to 12F), 135-cm nasojejunal feeding tube should be inserted, under endoscopic or fluoroscopic guidance, and postpyloric feeding commenced. Nutrition may be commenced at 20 ml/hr and gradually increased as for nasogastric feeding (see Figure 34-1). Regular flushing with water helps to prevent blockage of the tube, particularly when low rates of feed are utilized.
Adverse Effects
Apart from hyperglycemia—which should be treated with intravenous insulin—the metabolic consequences of overfeeding that were described earlier are uncommon with enteral nutrition. Diarrhea and constipation are common, each occurring in about 15% of enterally fed patients.24 Other commonly reported adverse effects include gastric stasis (39%), abdominal distention (13%), vomiting (12%), and regurgitation (5%).24 There is no difference in the incidence of aspiration between gastric and postpyloric feeding.25 Occasionally, a large volume (>1 to 2 l/day) of gastric fluid is aspirated from the stomach despite successful postpyloric feeding. If this fluid is discarded, hypovolemia and hypochloremic metabolic alkalosis can develop. The treatment is intravenous 0.9% saline. Intolerance of nasogastric nutrition is very common and is not necessarily a cause for concern; intolerance of postpyloric feeding is less common and may indicate intraabdominal pathology (see subsequent material).
Sinusitis can occur when nasogastric or nasojejunal feeding tubes are in situ for long periods. Polyurethane or silicone feeding tubes should be used when enteral feeding is anticipated to be used for longer than 2 weeks because polyvinylchloride tubes progressively degrade during contact with gastric contents.26
Parenteral Nutrition
Composition
Parenteral nutrition is provided in elemental form: nitrogen as L-amino acids, carbohydrate as glucose, and fat as fatty acids. The appropriate proportion of nitrogen, carbohydrate, and fat is the subject of debate, but a ratio similar to that used for enteral nutrition is common. The advantage of a relatively high proportion of fat is the avoidance of hyperglycemia secondary to high glucose administration; the disadvantage is a potentially increased incidence of nosocomial infection.27 If it is anticipated that parenteral nutrition will be required for fewer than 10 days in a patient who is not malnourished, withholding lipids should be considered.16 Vitamins and trace elements are added in appropriate amounts.
Variable amounts of sodium, potassium, calcium, magnesium, buffer, and water are added to suit patients’ needs. Many patients require water restriction, and a minimum volume of 1 liter per 24 hours is usually possible. Daily sodium and potassium requirements are discussed in Chapter 32. Many patients receiving parenteral nutrition have expanded extracellular spaces and require very little, if any, sodium. Potassium requirements may be high because of insulin treatment given for hyperglycemia or low due to renal failure. Anions are provided as a mixture of chloride and acetate, with a small amount of phosphate. Relatively more chloride may be used in patients with alkalosis, and relatively more acetate may be used in patients with acidosis.
Route of Administration
Parenteral nutrition is hypertonic and must be administered via a central venous catheter. To minimize the risk of infection, it should be a dedicated single-lumen catheter inserted either peripherally or into the subclavian vein (see Chapter 40). Three-way taps in the infusion set should be avoided, and the delivery tubing and any remaining nutrition should be changed each day using aseptic precautions.
Adverse Effects and Biochemical Testing
Hyperglycemia should be treated with intravenous insulin (see Chapter 36). Hypoglycemia can occur with abrupt cessation of treatment, so when it is no longer required, patients should be weaned from parenteral nutrition slowly over several hours. If for some reason the daily supply is interrupted, patients should be commenced on a dextrose infusion at a rate similar to the concentration in the parenteral nutrition.
Chronically malnourished patients who receive aggressive nutritional support, particularly via the intravenous route, are at risk of the refeeding syndrome.28,29 This condition is characterized by disturbances in the balance of body sodium and water (hypovolemia with predominantly protein feeding and hypervolemia with predominantly carbohydrate feeding), hypophosphatemia, hypokalemia, hypomagnesemia, and thiamine deficiency (manifested as Wernicke encephalopathy). Thiamine (100 mg intravenously daily for 3 days) should be given before commencing feeds if malnutrition is suspected. Profound hypophosphatemia can cause myopathy and rhabdomyolysis. Refeeding syndrome is very uncommon in postoperative cardiac surgery patients. Complications that involve vascular access devices are listed in Chapter 40.
INTRAABDOMINAL COMPLICATIONS
Diarrhea and Constipation
Diarrhea and constipation are common in hospitalized patients. Diarrhea is a common occurrence in patients receiving enteral nutrition,24 particularly when calorie-dense feeds (1.5 to 2.0 kcal/ml) are used. Adding nonabsorbable soluble fiber or changing to a more dilute feed may be beneficial. Once other causes of diarrhea have been excluded, antidiarrheal drugs such as loperamide or codeine may be used. An algorithm for treatment of diarrhea is provided in Figure 34-2.
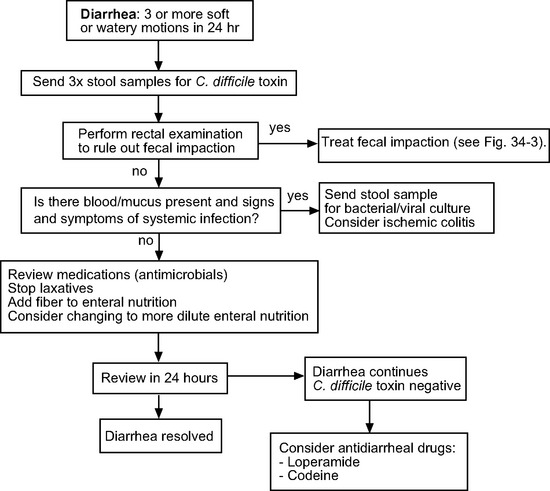
Bacterial overgrowth by Clostridium difficile, a gram-positive, anaerobic bacillus, may require specific treatment. Clostridium colitis is diagnosed by identifying C. difficile toxin in the stool. Risk factors include prolonged ICU stay and treatment with antimicrobials (particularly clindamycin, cephalosporins, and fluoroquinolones) and proton pump inhibitors. Usually, the condition causes diarrhea only. Rarely, pseudomembranous colitis, an inflammatory condition of the large bowel that is associated with toxic megacolon and bowel perforation, can result. If diarrhea is mild, no treatment is required other than stopping the offending antimicrobial. However, if diarrhea is severe or there are other abdominal symptoms and signs, treatment with metronidazole or oral vancomycin is indicated.30
Reduced frequency of bowel motions is normal following cardiac surgery due to reduced oral intake and the effect of opioid analgesics. However, if it is persistent and untreated, severe constipation or fecal impaction can develop. If patients have not had a bowel motion by postoperative day 2, and in the absence of contraindications, laxatives should be commenced. A protocol for the prevention and treatment of constipation is provided in Figure 34-3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


