Variable
Technique
What it means in cardiac sarcoidosis?
Resting myocardial perfusion imaging
Can be performed by either SPECT or PET myocardial perfusion imaging
Resting perfusion defects can be due to either scar and/or intense inflammation causing compression of the microvasculature
Imaging inflammation with F18 flurodeoxyglucose
Performed with PET
Following adequate patient preparation (see text), increased FDG uptake represents myocardial inflammation
Can be quantified
May improve upon treatment with systemic anti-inflammatory medications
Can be used to visualize areas of increased FDG uptake outside the heart
Requires suppression of glucose uptake by normal myocardium and exclusion of other causes of increased FDG uptake by the myocardium
While the use of rest MPI is extremely helpful when interpreting FDG PET images, the value of rest MPI alone imaging is limited. For instance, in early stages of cardiac sarcoidosis, the rest MPI can be completely normal. Among patients with suspected cardiac sarcoidosis, the presence of a resting perfusion defect is often non-specific as the differential diagnosis for this finding includes: (a) scar and/or inflammation from cardiac sarcoidosis; (b) artifact, such as an attenuation artifact; (c) scar from prior myocardial infarction; or (d) hibernating myocardium.
Inflammation Imaging Using F18-Flurodeoxyglucose
F18-FDG is used to image myocardial inflammation based on the fact that inflammatory cells such as macrophages have a higher metabolic activity. After crossing the cell membrane, F18-becomes phosphorylated by the enzyme hexokinase and then becomes trapped inside the cells, thus allowing for imaging. However, it is important to remember that FDG uptake by the myocardium is not specific to cardiac sarcoidosis, and must be interpreted in the context of the patient’s medical history as well as the dietary conditions that were employed at the time of image acquisition. For instance, patients with coronary heart disease who have hibernating myocardium (i.e. reduced perfusion due to chronic ischemia accompanied by a shift in metabolic pathways to favor glucose uptake instead of free fatty acids) may have FDG uptake. Other inflammatory myopathies, such as active myocarditis or systemic rheumatological conditions with cardiac involvement may also be associated with increased FDG uptake by the myocardium. Finally, FDG uptake by the myocardium – especially when diffuse or confined to the lateral wall – may be a normal variant, particularly when imaging is performed in the non-fasted state and/or under states of high insulin.
The Logistics of Performing FDG PET Imaging
Patient Preparation
Adequate patient preparation to suppress the physiologic uptake of FDG by the normal myocardium is essential when performing PET imaging for inflammation. There are multiple protocols (Table 6.2) that have been used by different centers and no clear data to support the superiority of any one particular method. Cheng et al. studied 63 patients referred for oncologic imaging, and found that a low carbohydrate diet followed by a fast resulted in greater reduction in SUV (versus a controlled group of patients following an unrestricted diet) than a high fat low carbohydrate diet in which patients also drank a 250 cc beverage of mostly non-saturated fat 1 h prior to FDG injection [7]. Recently, Demeure et al. showed that a high fat low carbohydrate diet followed by a 12 h fast effectively suppressed FDG uptake in most (8 out 9) subjects. In their study, and consistent with the results of Cheng et al. administering an extra fat load 1 h before the scan did not offer any benefit [8]. Based on these two studies, administering a high fat beverage prior to imaging is not recommended. It is possible that such an approach of overloading the myocardium with free fatty acids could increase myocardial oxygen consumption leading to a paradoxical increase in glucose metabolism. In general, even under optimal conditions, approximately 10 % of patients may have diffuse non-specific uptake of FDG by the myocardium.
Table 6.2
Methods used to suppress FDG from the normal myocardium
Protocol | Comments/tips |
|---|---|
High fat low carbohydrate diet × 2 meals followed by fast of at least 4 h | Good experience by our group; used in Blankstein et al. [9] |
High fat low carbohydrate (HFLC) diet + prolonged fast | Supported by Demeure et al. [8] |
Low carbohydrate (LC) diet followed by fast | Supported by Cheng et al. [7] |
Prolonged fast | Suggest at least 18 h fast |
Supported by Morooka et al. [15] | |
High fat low carbohydrate diet supplemented by high fat beverage 1 h prior to FDG injection | |
Heparin administration | Dose 50 IU/kg used in some studies, but lower doses may also be effective (avoid administering in dextrose); inferior to long term fasting [15] |
At our center we recommend a high fat/low carbohydrate diet for two meals prior to the scan followed by a fast of at least 4 h. Prior to imaging, all patients are asked about their diet, and if there are any issues (i.e. patient inadvertently ate carbohydrates), the study is postponed. In addition, patients are asked to avoid any strenuous exercise for 1 day prior to the scan. In patients who are unable to follow this diet (e.g. NPO for other medical reasons) we suggest a prolonged fast of at least 18 h.
Imaging Protocol
FDG image acquisition is typically performed 90 min after the administration of 10–12 mCi of F18-FDG although a shorter uptake period of 60 min has also been used by some centers. Our suggested protocol includes:
1.
Low dose CT images for attenuation correction
2.
Whole body FDG imaging – imaging from cerebellum to thigh utilizing multiple bed acquisitions performed in 3D (approximately four to five bed acquisitions are needed, depending on patient’s height as well as z-axis coverage per bed position)
3.
Cardiac FDG imaging – single bed 3D acquisition over the heart with longer acquisition duration (~10 min)
Whole body FDG is an important component of the cardiac PET exam as this information can identify the presence and severity of extra cardiac disease. When present, such disease may help inform the role of anti-inflammatory therapies. In addition, when the diagnosis of sarcoidosis is uncertain, the presence of extra cardiac FDG avid disease may identify potential biopsy targets that are more accessible than the heart. These images should be interpreted by a physician who is trained at body PET/CT as it is important to recognize normal distribution of FDG by various organs from pathologic uptake.
Image Interpretation
Image interpretation requires simultaneous visualization of both rest MPI and FDG PET images. Normal scans will have complete suppression of FDG from the myocardium with normal resting perfusion (Fig. 6.1). At times, patients without cardiac disease may also have diffuse homogenous uptake of FDG by the myocardium. This pattern should be distinguished from diffuse patchy myocardial involvement which can be seen in patients with extensive myocardial inflammation.
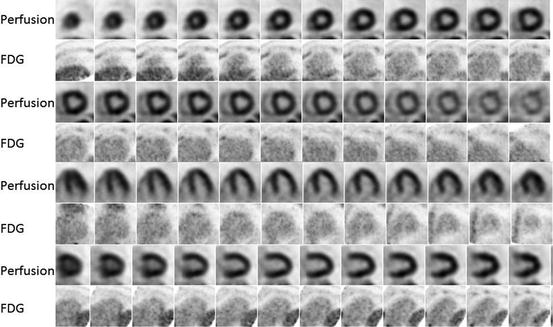




Fig. 6.1
Example of normal F-18 FDG PET/CT. Rest myocardial perfusion imaging demonstrates normal perfusion of the left ventricle with no defects. The cardiac FDG images show good suppression of FDG from the myocardium with no focal uptake involving the left or right ventricles
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
