Chapter 7
Nuclear Cardiology
1. What is nuclear cardiology?
2. What is myocardial perfusion imaging (MPI)?
3. Define a perfusion defect and differentiate between a reversible and fixed defect.
A perfusion defect is an area of reduced radiotracer uptake in the myocardium.
If the perfusion defect occurs during stress and improves or normalizes during rest, it is termed reversible (Fig. 7-1). Generally, a reversible perfusion defect suggests the presence of ischemia.
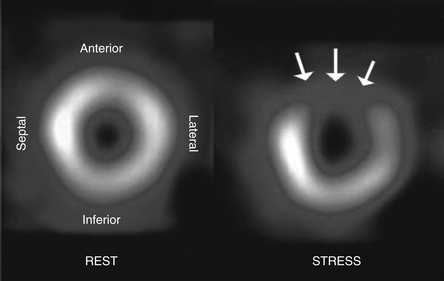
Figure 7-1 Nuclear stress testing short-axis view demonstrating a reversible perfusion defect. Normal myocardial perfusion occurred during resting images (left panel), but a large anterior wall perfusion defect (arrows) was seen during previous stress imaging (right panel). (Modified from Texas Heart Institute Website: Nuclear stress test. Available at http://www.texasheartinstitute.org/HIC/Topics/Diag/dinuc.cfm. Accessed March 22, 2013.)
4. What are the different uses of MPI?
 MPI is used to diagnose coronary artery disease (CAD) in patients with intermediate risk for CAD who present with chest pain or its equivalent.
MPI is used to diagnose coronary artery disease (CAD) in patients with intermediate risk for CAD who present with chest pain or its equivalent.




5. Is MPI the most sensitive and specific test for diagnosing CAD?
6. List the different perfusion agents used in MPI.
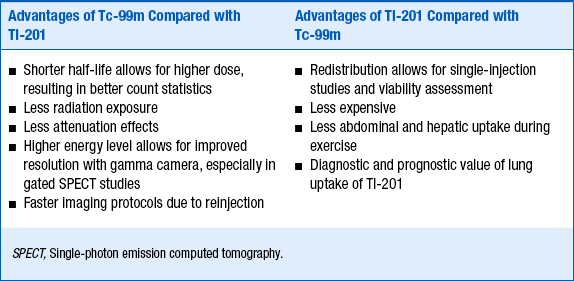
For an agent to be an effective radiopharmaceutical, its distribution has to be proportional to regional blood flow, have a high level of extraction by the organ of interest, and have rapid clearance from the blood. The two most important physiologic factors that affect myocardial uptake of a radiotracer are variations in regional blood flow and the myocardial extraction of the radiotracer. In other words, there will be more uptake of a radiotracer in areas of increased blood flow and less in areas supplied by diseased or stenosed vessels. Importantly, because myocardial extraction is an active process with regard to thallium-201 and a mitochondrial-dependent process with regard to the technetium-99m agents, it can only occur if the cells in that region are viable. The relative advantages and disadvantages of thallium-201 and technitium-99 are summarized in Table 7-1.