Chapter 2
Not Just ‘Small Adults’: Paediatric Anatomy and Physiology in Relation to Trauma
Written by B.M. Morrow
Children cannot be considered merely as ‘small adults’. Children are fundamentally different in terms of cognitive, physical and psychological development, anatomy and physiology. For the purposes of this textbook, the term ‘paediatric’ includes infants, children and adolescents up to the age of 16 years.
In this chapter information is shared about:
•The anatomical and physiological differences between the adult and child in relation to:
 The airway.
The airway.
 The chest, lungs and breathing.
The chest, lungs and breathing.
 The heart and circulation.
The heart and circulation.
 The head, neck and central nervous system.
The head, neck and central nervous system.
 The abdomen.
The abdomen.
 The musculoskeletal system.
The musculoskeletal system.
 Temperature regulation.
Temperature regulation.
2.1. Introduction
Trauma is a significant contributor to childhood mortality and morbidity. In most developed countries, in which less than 20% of the population is under 15 years of age, trauma is the main cause of childhood mortality (Bayreuther et al., 2009). In developing countries, in which children represent almost half the population, trauma has an even bigger impact on child health (Van As and Rode, 2006). It is estimated that more than 95% of all injury-related deaths in children occur in low and middle-income countries. This is at least partly explained by inadequate adult supervision and exposure to hazardous environments (e.g. traffic, unsafe play areas, cramped living conditions with open fires and unprotected windows (absence of burglar bars or mesh covered windows)).
The nature of activities at different maturation and neuro-developmental stages (with changing levels of independence) predispose infants, children and adolescents to different patterns of injury to those of adults. Children inhabit a different physical zone to adults; they are closer to the ground, and potentially also closer to a number of associated hazards which are not a problem to the taller adult. Young children are inquisitive and know no fear; they climb, squeeze into small spaces and pull things down from high surfaces to investigate them (WHO, 2008a).
Pre-ambulatory children (toddlers) cannot remove themselves from a dangerous situation or environment; such youngsters do not have sufficient judgement to recognise potentially dangerous situations. Additionally, pre-reading children cannot read warning signs to alert them to possible hazards, and pre-adolescent and adolescent children may take unreasonable risks due to cognitive immaturity and normal ‘risk-taking’ behaviours. Boys tend to have more frequent and more severe injuries than girls, possibly due to greater risk-taking activities, higher activity levels, more impulsive behaviour and less social restriction than girls (Miller et al., 2002; WHO, 2008a).
Whilst adults are frequently involved in industrial or other work-related accidents and motor vehicle accidents, common injuries in children relate to falls and playground accidents. Even when experiencing the same accident as their adult counterparts, infants and children may present with substantially different injuries. For example, a pedestrian vehicle accident involving an adult will frequently result in fractured long bones (because of the taller stature), whereas a child may present with abdominal or thoracic injuries (Crameri, 2010).
Being dependent on adults unfortunately also puts infants and children at risk of abuse. Physiotherapists treating young children should be aware of the potential for non-accidental injury (NAI), and report it promptly should the child or caregiver disclose any suspicious circumstances or if the examination yields concerning findings. Care should be taken that physiotherapy intervention is not seen as a perpetuation of physical abuse.
2.2. Anatomical and Physiological Differences between the Adult and Child
2.2.1. General
The smaller the child, the greater the likelihood that a single traumatic impact will injure multiple organ systems. When exposed to intense heat, delicate infant skin burns more quickly and to a greater depth than the thicker skin of adults (WHO, 2008b).
2.2.2. The airway
Children are significantly different to adults in their upper airways (Fig. 2.1). The tongue is relatively larger in a child than in an adult and the oral cavity is relatively smaller. The tongue is therefore more likely to obstruct the airway than in an adult. Correct positioning of the head and jaw is therefore imperative to ensure airway patency during resuscitation (Fig. 2.2) (Santillanes and Gausche-Hill, 2008; Crameri, 2010; Harless et al., 2014).
Infants are obligatory nose breathers for the first four to six months of age, in order to allow them to suck and breathe simultaneously. They are therefore more prone to experiencing respiratory compromise if the nose is blocked (by blood or mucus for example). By five to six months of age, infants can take occasional effective oral breaths, and by eight months they are able to breathe normally through the mouth (Santillanes and Gausche-Hill, 2008; Crameri, 2010).
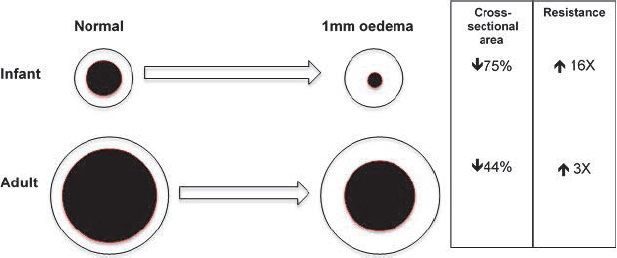
The paediatric airway has a smaller diameter than that of an adult and is very compliant with poor support by surrounding structures. This predisposes the infant to airway obstruction. By Poiseuille’s Law, resistance is inversely proportional to the fourth power of the radius. Therefore, a small change in airway diameter has a large impact on overall airway resistance (Fig. 2.3). A small amount of swelling can cause significant obstruction, with resulting increases in airway resistance and work of breathing. If the radius is halved, then resistance increases 16 times. Only by the age of eight does the paediatric airway function in a similar manner to the adult airway (Santillanes and Gausche-Hill, 2008; Crameri, 2010).
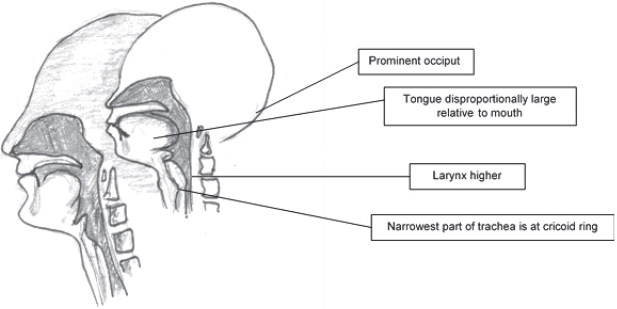
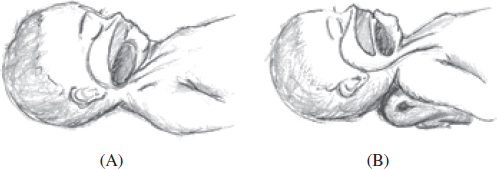
Fig. 2.2:Airway opening (sniffing position) in an infant. The large occiput in image (A) causes head flexion, which leads to obstruction of the upper airway by the base of the tongue. In image (B) placing a towel roll under the shoulders has increased neck extension, thus relieving the obstruction.
Foreign body aspiration is common in children, particularly those with loose deciduous teeth. Aspiration of a small object can lead to significant airway compromise due to the small diameter of the central airways (Crameri, 2010).
The trachea is cartilaginous and more pliable than in an adult, making it easy to collapse and obstruct. The paediatric trachea is also comparatively shorter than that of the adult, which increases the risk of accidental extubation. Large tonsils in young children may also contribute to airway obstruction and make intubation difficult (Santillanes and Gausche-Hill, 2008).
The larynx is higher and more anterior (at the level of the 2nd–3rd cervical vertebrae) in the young child, compared with the 6th–7th cervical vertebrae in the adult (Fig. 2.1). This makes visualisation of the larynx more difficult in the paediatric airway, which also has implications for intubation (Crameri, 2010).
The epiglottis of the young child is horseshoe-shaped and projects posteriorly at 45°. Again, this makes intubation more difficult.
The cricoid ring is the narrowest point in the airway in children and this region is lined with a delicate epithelium which is easily injured, leading to oedema. Therefore, an uncuffed endotracheal tube is usually used in cases of paediatric trauma in order to prevent subglottic stenosis (Santillanes and Gausche-Hill, 2008; Crameri, 2010).
2.2.3. The chest, lungs and breathing
The ribs of infants are cartilaginous and are positioned more horizontally than those of adults, with a resulting barrel-shaped chest (Figs 2.4 and 2.5). Although the intercostal muscles are present and functional, the position of the ribs confers a mechanical disadvantage to intercostal contraction and the diaphragm is therefore the main muscle of respiration in infants and young children. The resulting rib excursion is therefore limited, which in turn limits the capacity to increase tidal volumes.
Because the diaphragm is the main respiratory muscle, any increase in abdominal pressure (e.g. abdominal distension) will impact on respiratory function. Decompression of the stomach is important after trauma to prevent a distended abdomen from impinging on diaphragmatic excursion. The paediatric diaphragm also has fewer type 1 (fatigue-resistant) muscle fibres than in adults and is therefore prone to fatigue (Santillanes and Gausche-Hill, 2008; Crameri, 2010).
The chest wall is more compliant than adults, but the lungs are relatively less compliant. As a result of this increased elasticity of the chest wall, blunt chest trauma may not result in rib fractures in the infant and young child. However, the force may be transmitted through the cartilaginous ribs to the underlying structures, potentially causing significant internal injuries. Small children are more susceptible to pneumothoraces on the application of positive pressure. Infants tire quicker and more easily than adults, so early aggressive intervention may be needed to protect the airways and maintain ventilation. Early signs of respiratory distress can deteriorate very rapidly, so close observation is required (Kadish, 2006; Escobar and Caty, 2011).
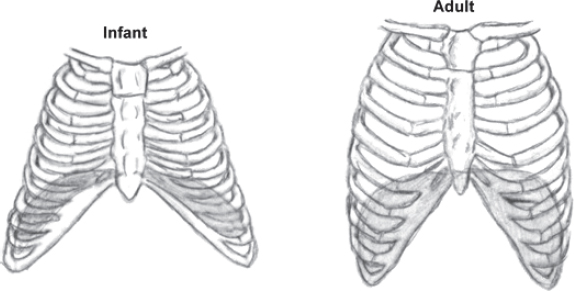
Fig. 2.4:Position of ribs and diaphragm in paediatric versus adult thorax.

Fig. 2.5:Chest x-ray of a three-week-old infant, showing horizontal ribs and relatively flatter diaphragm.
The highly compliant chest wall provides little support for the lungs, thus the negative intrathoracic pressure is poorly maintained and the work of breathing can increase to approximately three times that of the adult.
The number and size of alveoli increase from 20–50 million alveoli at birth until about 300 million alveoli at eight years of age. Young children therefore have less surface area for gaseous exchange than adults. The collateral ventilatory channels are also poorly developed in young children, predisposing them to atelectasis (Charnock and Doershuk, 1973; WHO, 2008a) (Fig. 2.6).
It has long been taught that children have a different pattern of ventilation to adults: whereas adults uniformly preferentially ventilate the dependent lung, children were thought to preferentially ventilate the non-dependent lung, and this pattern was said to continue well into the second decade of life (Davies et al., 1985; Bhuyan et al., 1989; Davies et al., 1992). More recent studies using electrical impedance tomography in infants under six months of age (Frerichs et al., 2003; Schibler et al., 2009) and older infants and children (Lupton-Smith et al., 2014) have refuted this hypothesis. Neonates appear to have a similar pattern of ventilation to adults, while the distribution of ventilation in both spontaneously breathing and mechanically ventilated older infants and children is highly variable (Lupton-Smith et al., 2014; Lupton-Smith et al., unpublished data). Further studies are required to determine what factors influence the pattern of ventilation in children, but individual assessment of response to treatment is recommended, rather than prescribing standard positions for specific lung zones.
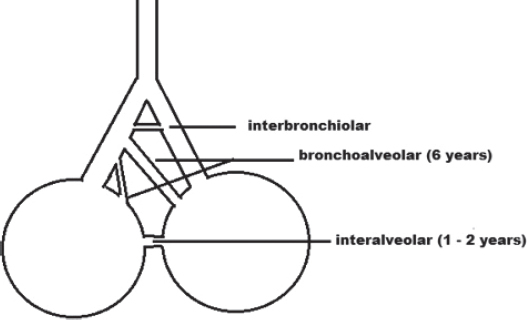
Fig. 2.6:Development of collateral ventilation channels (interbronchiolar channels of Martin; bronchoalveolar channels of Lambert; interalveolar pores of Kohn).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


