Fig. 2.1
Celiac artery anatomy and superior mesenteric artery collaterals. CA celiac artery, SMA superior mesenteric artery (By permission of Mayo Foundation for Medical Education and Research. All rights reserved)
The left gastric artery may originate from the aorta or anywhere along the celiac artery. It travels superiorly supplying the distal esophagus and then descends along the lesser curvature of the stomach to collateralize with the right gastric artery (Figs. 2.1 and 2.2a). Importantly, the left hepatic artery may be replaced, originating from the left gastric. When present, it is important to preserve this during access to the supraceliac aorta though the lesser sac. Conversely, the left hepatic artery may supply an accessory left gastric artery.

Fig. 2.2
Gastric and bowel collateral networks. (a) Gastric collaterals. Right and left gastric arteries collateralize along the lesser curvature, while the right and left gastroepiploic arteries collateralize along the greater curvature of the stomach. (b) Celiac to superior mesenteric artery (SMA) collaterals include the arch of Bühler and gastroduodenal arcade. SMA to inferior mesenteric artery (IMA) collaterals include the arc of Riolan and the marginal artery of Drummond. Perirectal collaterals form from the IMA, superior rectal artery, and internal iliac artery (By permission of Mayo Foundation for Medical Education and Research. All rights reserved)
The splenic artery originates from the celiac artery 80 % of the time. As the splenic artery traverses to the left, it gives off segmental branches to the pancreas (the dorsal pancreatic and caudal pancreatic arteries). These supply the body and the tail of the pancreas, respectively, collateralizing via the transverse pancreatic artery (Fig. 2.1). Distal branches of the splenic artery include the short gastric arteries, posterior gastric, left gastroepiploic, and the terminal splenic branches. The short gastric arteries number from 1 to 4 and collateralize to the greater curvature of the stomach and the aforementioned left gastric artery. The posterior gastric artery supplies the posterior fundus of the stomach. The left gastroepiploic artery often arises from the distal splenic artery in a common branch with the inferior splenic branch but may be a single branch. It travels along the greater curvature of the stomach giving off omental branches and collateralizing with the right gastroepiploic artery (Figs. 2.1 and 2.2a).
The common hepatic artery is the final branch of the celiac artery. It is of variable length and ends at the gastroduodenal artery branch, after which it continues as the proper hepatic artery to supply the liver and gallbladder. The proper hepatic artery bifurcates into the right and left hepatic arteries (Fig. 2.1). Alternatively, there may be a trifurcation of the common hepatic artery with no proper hepatic artery. The proper hepatic artery or only the right hepatic may arise from the SMA as variants. As mentioned, the left hepatic artery may arise from the left gastric artery. The right gastric artery may arise anywhere along the common or proper hepatic artery to collateralize along the lesser curvature with the left gastric artery (Figs. 2.1 and 2.2a).
The gastroduodenal artery passes inferiorly between the duodenum and the pancreas, giving rise to the right gastroepiploic artery and the superior pancreaticoduodenal artery. This has anterior and posterior divisions that are important collaterals to the superior mesenteric artery (Figs. 2.1 and 2.3).
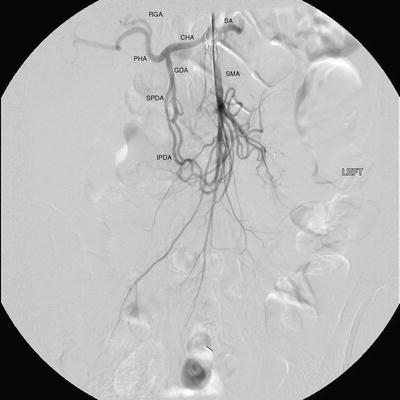
Fig. 2.3
Celiac artery and superior mesenteric artery collaterals. CHA common hepatic artery, SA splenic artery, RGA right gastric artery, PHA proper hepatic artery, GDA gastroduodenal artery, SMA superior mesenteric artery, SPDA superior pancreaticoduodenal artery, IPDA inferior pancreaticoduodenal artery
Superior Mesenteric Artery (SMA)
The SMA is the second ventral branch of the abdominal aorta. As mentioned above in the discussion of embryology, this artery will supply the distal duodenum, the small intestine, and the large intestine to the mid transverse colon. Given the vitally important structures its supplies and the important collaterals it provides to both the celiac and IMA, there is a very high morbidity associated with SMA occlusions. Anatomically, the SMA origin is about a centimeter distal to the celiac artery and accessible through the lesser sac near the superior border of the pancreas. The SMA comes off at an acute angle in comparison to the celiac artery. In this aortomesenteric angle, the left renal vein and the fourth portion of the duodenum pass. If this angle is too acute, it may lead to either nutcracker syndrome or SMA syndrome. Symptoms include flank pain and hematuria related to renal vein compression for the former and a gastric outlet obstruction syndrome related to the latter.
SMA branches include [2]:
1.
Inferior anterior and posterior pancreaticoduodenal arteries
2.
Middle colic artery
3.
Right colic artery
4.
Ileocolic artery
5.
Jejunal and ileal branches
The first branches of the SMA include the inferior pancreaticoduodenal artery. This comes off the right side of the SMA and divides in to an anterior posterior branch that collateralize to the celiac artery via the previously mentioned collateral pathway (Figs. 2.1, 2.2, and 2.3). The middle colic artery arises from the proximal SMA after passing below the pancreas. This artery travels to the transverse mesocolon giving a right and left branch. During an infracolic exposure of the SMA, when this artery is identified within the transverse mesocolon, it can be followed down to identify the SMA. Within the mid SMA, the right colic artery originates. It is the last branch off the right side of the SMA. As the right colic artery traverses behind the parietal peritoneum, its supplies a descending and ascending branch. The ascending branch collateralizing with the middle colic artery and supplies the ascending right colon. The descending branch collateralizes to the ileocolic artery, supplying the more proximal right colon (Figs. 2.4 and 2.5).
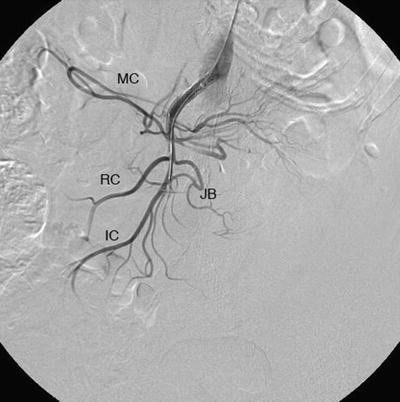
Fig. 2.4
Superior mesenteric artery and inferior mesenteric artery anatomy and collaterals. SMA superior mesenteric artery, IMA inferior mesenteric artery, IC ileocolic artery, RC right colic artery, MC middle colic artery, LC left colic artery, SA sigmoid arteries, SR superior rectal artery. The marginal artery of Drummond is formed by the arterial network from the ileocolic to the superior rectal. Critical regions of collateralization include Griffith’s point (SMA to IMA) and Sudeck’s point (IMA to internal iliac artery) (By permission of Mayo Foundation for Medical Education and Research. All rights reserved)
Fig. 2.5
Superior mesenteric artery angiographic anatomy. IC ileocolic artery, RC right colic artery, MC middle colic artery, JB jejunal branches
The ileocolic artery is the final major branch of the SMA but may share a common origin with the right colic artery. The ileocolic artery vascularizes the terminal ileum, right colon, cecum, and appendix. There are four identifiable branches. These included the descending branch (to the right colon), cecal branch (an anterior and posterior), ileal branch, and the appendicular artery (to the appendix). Finally, on the left aspect of the SMA arise the multiple jejunal and ileal branches. These fan out, forming several arches to create a collateralized network to the small bowel (Figs. 2.4 and 2.5).
Inferior Mesenteric Artery
The inferior mesenteric artery is responsible for supplying blood flow to the distal third of the transverse colon, descending colon, sigmoid colon, as well as the upper rectum. It originates in an anterior lateral orientation to the left just above the aortic bifurcation, typically between the L2 and L4 vertebral bodies [3]. It travels in a retroperitoneal plane towards the sigmoid colon.
The left colic artery is comprised of an ascending and descending branch. The ascending collateralizes to the middle colic artery, distal transverse colon, and splenic flexure (Griffith’s point [4], Fig. 2.4). This collateralization is important, as this area is at high risk for watershed ischemia in the setting of dehydration or mesenteric occlusive disease. The descending left colic artery branch collateralizes to the sigmoid arteries. These are comprised of two or three sigmoid artery branches within the mesocolon. The uppermost sigmoid artery collateralizes to the left colic artery, whereas the lowermost collateralizes to the superior rectal artery. The superior rectal artery descends into the pelvis dividing into right and left branches. The superior rectal artery collateralizes with both the middle rectal (branch of the internal iliac artery) and the inferior rectal artery (branch of the internal pudendal artery, Fig. 2.4).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


