TABLE 155.1 Types of Congenitally Anomalous Coronary Arteries | |||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||
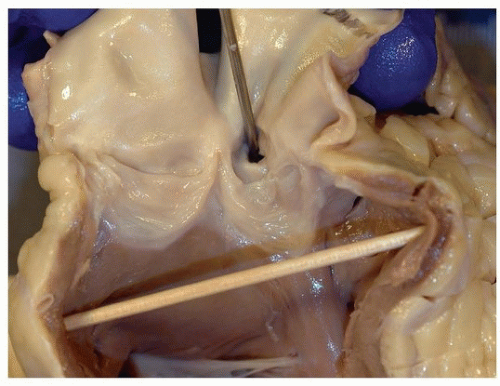 FIGURE 155.1 ▲ Anomalous origin, pulmonary trunk. The probe is inserted into the left main ostium, which arose in the anterior sinus of the pulmonary valve. |
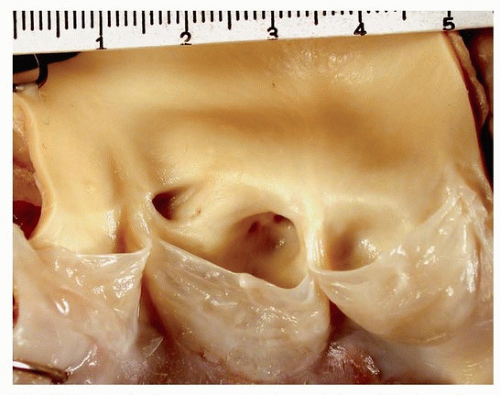 FIGURE 155.2 ▲ Anomalous origin, left main from right sinus of Valsalva. Note the left main ostium just to the right of the commissure, in the same sinus as the right (right sinus of Valsalva). |
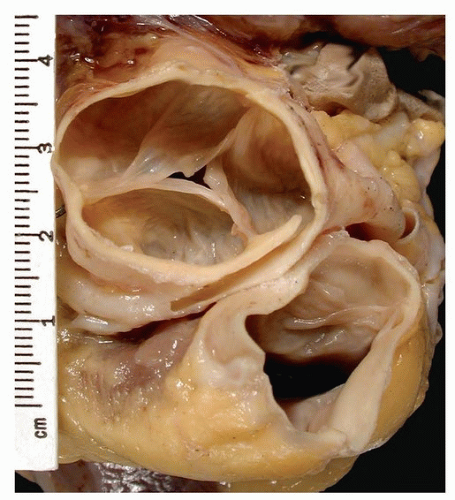 FIGURE 155.3 ▲ Anomalous origin, right coronary from the left sinus of Valsalva. Viewed from above, note the right artery arising from the left sinus of Valsalva. The pulmonary trunk is below and to the right. There is a long course between great vessels, which may become compressed during diastole when the artery normally fills. |
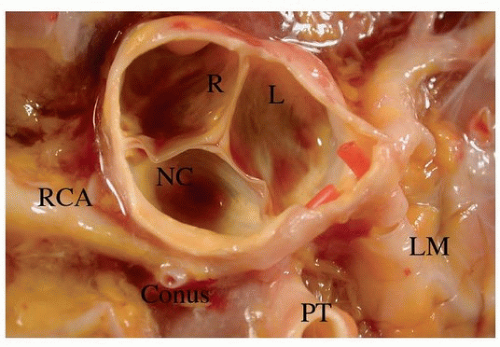 FIGURE 155.4 ▲ Anomalous origin, right coronary from the left sinus of Valsalva. There are red plastic tubes present within the ostia. The left main (LM) is normal, whereas the right coronary artery (RCA) arises from the left sinus to the left of the pulmonary trunk (PT). R, right sinus of Valsalva; L, left sinus of Valsalva; NC, noncoronary sinus. |
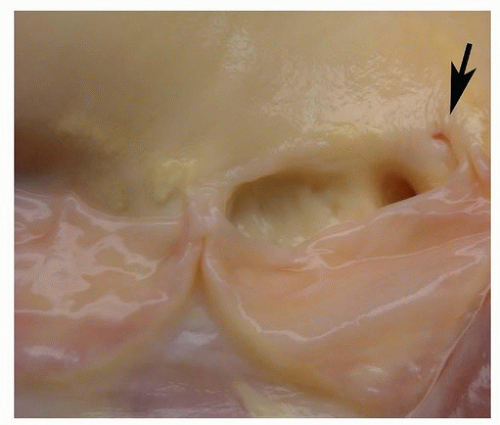 FIGURE 155.5 ▲ Anomalous origin, right coronary from the left sinus of Valsalva. In the left sinus of Valsalva, there are two ostia, one compressed (arrow) (anomalous right). |
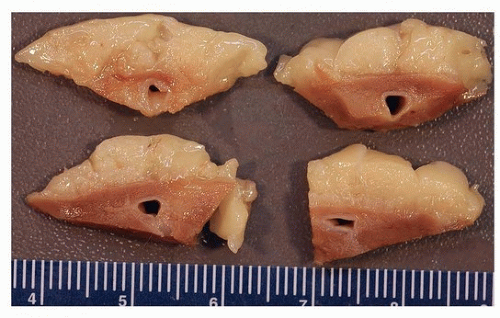 FIGURE 155.6 ▲ Tunnel coronary artery. The left anterior descending artery is separated from the epicardial fat by a rim of cardiac muscle. |
 FIGURE 155.7 ▲ High takeoff, left coronary ostium. The ostium is normally within the sinus under (proximal to) the sinotubular junction; in this example, it is above (distal to) the sinotubular junction, which is the area along the aortic annulus. |
evaluation is indicated, in order to distinguish congenital ostial stenosis to that caused by vasculitis, especially Takayasu disease, or coronary atherosclerosis.
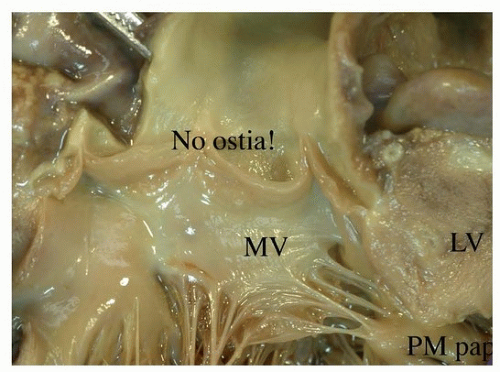 FIGURE 155.8 ▲ Absence of coronary ostia. In this infant’s heart, there was atresia of the ostia, secondary to complex congenital heart disease (pulmonary atresia with intact ventricular septum). MV, mitral valve; LV, left ventricular outflow; PM pap, posteromedial papillary muscle. |
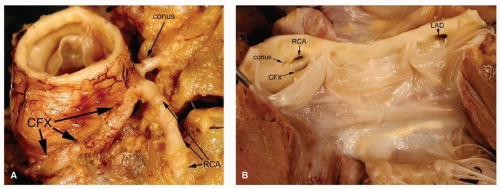 FIGURE 155.9 ▲ Anomalous origin of the left circumflex artery. A. This benign condition occurs when the left circumflex artery (CFX) arises from the right sinus near the ostium of the right coronary artery (RCA). In this case, there was a separate ostium for the conus artery, the first branch of the right coronary, also a benign condition. B. The valve is opened, demonstrating the ostia of the left circumflex (CFX), right coronary artery (RCA), and conus artery, all within the right sinus. The left main (LM) ostium is in the left sinus. LAD, left anterior descending. |
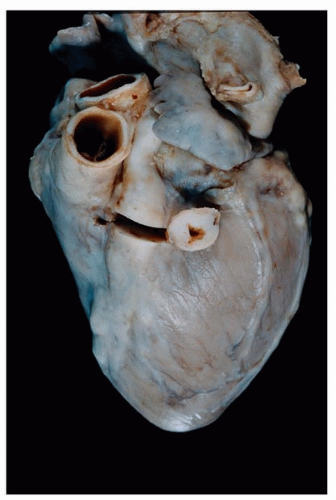 FIGURE 155.10 ▲ Kawasaki disease, adult aneurysm. There is an aneurysm of the proximal left anterior coronary artery with intimal thickening. The circumflex artery is also prominent. (Figure courtesy William Edwards, M.D.) |
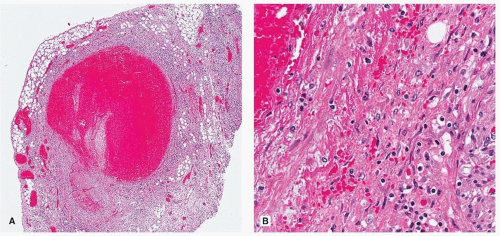 FIGURE 155.11 ▲ Kawasaki disease, acute-phase aneurysm. The patient, a 3-year-old child, died from complications of mucocutaneous lymph node syndrome and hemophagocytic lymphohistiocytosis, an uncommon association. A. At low magnification, there is ectasia of the artery with occlusive thrombus. B. The media shows chronic inflammation and thinning. There is no fibrinoid necrosis, as would be present in necrotizing arteritis such as polyarteritis nodosa. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


