Chapter 17
Non–ST Segment Elevation Acute Coronary Syndrome
1. What is non–ST segment elevation acute coronary syndrome?
It is now recognized that unstable angina, non–Q wave myocardial infarction (MI), non–ST segment elevation MI, and ST segment elevation myocardial infarction (STEMI) are all part of a continuum of the pathophysiologic process in which a coronary plaque ruptures, thrombus formation occurs, and partial or complete, transient or more sustained vessel occlusion may occur (Fig. 17-1). This process is deemed acute coronary syndrome when it is clinically recognized and causes symptoms. Acute coronary syndromes can be subdivided for treatment purposes into non–ST segment elevation acute coronary syndrome (NSTE-ACS) and ST segment elevation acute coronary syndrome (STE-ACS).
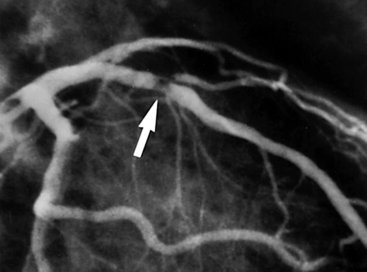
Figure 17-1 Plaque rupture in the proximal left anterior descending (LAD) coronary artery has led to thrombus formation (arrow) and partial occlusion of the vessel. (Reproduced with permission from Cannon CP, Braunwald E: Unstable angina and non–ST elevation myocardial infarction. In Libby P, Bonow R, Mann D, et al, editors: Braunwald’s heart disease: a textbook of cardiovascular medicine, ed 8, Philadelphia, 2008, Saunders, p. 1179)
2. What is the current definition of a myocardial infarction?


 Development of pathologic Q waves in the ECG
Development of pathologic Q waves in the ECG
 Imaging evidence of new loss of viable myocardium or new regional wall motion abnormalities
Imaging evidence of new loss of viable myocardium or new regional wall motion abnormalities
3. What other conditions besides epicardial coronary artery disease and acute coronary syndrome can cause elevations in troponin?
Although troponins have extremely high myocardial tissue specificity and sensitivity with new assay, numerous conditions besides epicardial coronary artery disease and acute coronary syndromes may cause elevations of troponins. Such conditions include noncoronary cardiac disease (myocarditis, acute congestive heart failure [CHF] exacerbation, cardiac contusion, apical ballooning syndrome), acute vascular pathology (hypertensive crisis, aortic dissection, pulmonary embolus), infiltrative diseases (amyloidosis, sarcoidosis), and systemic illnesses (anemia, chromic kidney disease [CKD], hypothyroidism, hypoxemia). Conditions that have been associated with elevation of troponin levels are given in Table 17-1.
TABLE 17-1
CONDITIONS OTHER THAN CORONARY ARTERY DISEASE ASSOCIATED WITH ELEVATION IN CARDIAC TROPONIN
| System | Causes of Troponin Elevation |
| Cardiovascular | Acute aortic dissection Arrhythmia Medical ICU patients Hypotension Heart failure Apical ballooning syndrome Cardiac inflammation Endocarditis, myocarditis, pericarditis Hypertension Infiltrative disease Amyloidosis, sarcoidosis, hemochromatosis, scleroderma Left ventricular hypertrophy |
| Myocardial injury | Blunt chest trauma Cardiac surgeries Cardiac procedures Ablation, cardioversion, percutaneous intervention Chemotherapy Hypersensitivity drug reactions Envenomation |
| Respiratory | Acute PE ARDS |
| Infectious/Immune | Sepsis/SIRS Viral illness Thrombotic thrombocytopenic purpura |
| Gastrointestinal | Severe GI bleeding |
| Nervous system | Acute stroke Ischemic stroke Hemorrhagic stroke Head trauma |
| Renal | Chronic kidney disease |
| Endocrine | Diabetes Hypothyroidism |
| Musculoskeletal | Rhabdomyolysis |
| Integumentary | Extensive skin burns |
| Inherited | Neurofibromatosis Duchenne muscular dystrophy Klippel-Feil syndrome |
| Others | Endurance exercise Environmental exposure Carbon monoxide, hydrogen sulfide |
Reproduced with permission from Januzzi JL Jr: Causes of Non-ACS Related Troponin Elevations. Available at http://www.cardiosource.org. Accessed February 16, 2013.
4. What are the factors that make up the Thrombolysis in Myocardial Infarction (TIMI) Risk Score?

 Three or more risk factors for coronary artery disease (CAD)
Three or more risk factors for coronary artery disease (CAD)
 Prior catheterization demonstrating CAD
Prior catheterization demonstrating CAD

 Two or more anginal events within 24 hours
Two or more anginal events within 24 hours
 Acetylsalicylic acid (ASA) use within 7 days
Acetylsalicylic acid (ASA) use within 7 days

5. What are the components of the Global Registry of Acute Coronary Events (GRACE) ACS Risk Model (at the time of admission)?
The components of the GRACE ACS Risk Model at the time of admission consist of:








Scores are calculated based on established criteria. Calculation algorithms are easily downloadable to computers and handheld devices. A low-risk score is considered 108 or less and is associated with a less than 1% risk of in-hospital death. An intermediate score is 109 to 140 and is associated with a 1% to 3% risk of in-hospital death. A high-risk score is greater than 140 and associated with a more than 3% risk of in-hospital death.
6. What other biomarkers and measured blood levels have been shown to correlate with increased risk of adverse cardiovascular outcome?
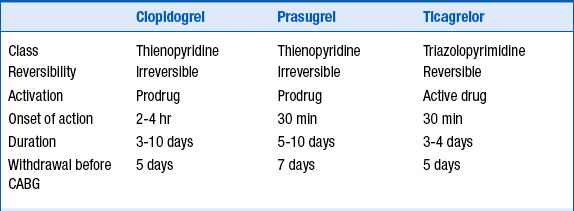
7. What are the differences between the oral antiplatelet agents?
More recently, the thienopyridine prasugrel and the triazolopyrimidine ticagrelor have been approved for use. These two agents have been studied in patients with ACS undergoing stent implantation. Like clopidogrel, both are P2Y12 blockers. Both these newer agents are more potent than clopidogrel, leading to greater and more reliable platelet inhibition than clopidogrel. They also both have a shorter onset of action than clopidogrel. Like clopidogrel, prasugrel irreversibly inhibits the platelet. Although ticagrelor does not irreversibly inhibit the platelet, there nevertheless is effective platelet inhibition for days following discontinuation of ticagrelor. The characteristics of these 3 agents are summarized in Table 17-2.