• No scars, less pain, earlier mobility and recovery
• Less physiological and psychological trauma
• Feasible alternative to surgery in co-morbid patients
• More ambulatory procedures
• Less overall cost associated with operative care
• Potential to offer therapy outside the operating room environment
Also, surgeons’ perceptions have been studied. The majority (72%) of the 357 surgeons who responded to a survey would be interested in becoming trained in NOTES. Predictors of surgeons being interested in NOTES included age less than 60 years, minimally invasive surgical subspecialty and flexible endoscopy used in more than 10% of the surgeons’ cases. The majority of the surgeons believed that NOTES took greater skill to perform and carried a greater risk of complications than laparoscopy, but it would be associated with less pain and faster recovery. About 56% of the surgeons would not prefer to perform cholecystectomy by NOTES; however, most felt they would switch to NOTES if data suggested improved outcomes compared with laparoscopy.
NOSCAR
The skills needed for the safe practice of NOTES cross two specialities: surgery and gastroenterology. For the successful development of this new technique, close collaboration between the two specialities is mandatory. In 2005, 14 leaders from the American Society of Gastrointestinal Endoscopy (ASGE) and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) met in New York City to discuss how to develop NOTES from theory into practice safely and efficiently and addressed the challenges, the limitations and the requirements in a white paper published in Surgical Endoscopy. The main goal was to harmonise research and progress in this field and to avoid the pitfalls which were associated with the overly hasty introduction of laparoscopic procedures for certain indications. Recommendations by the working group Natural Orifice Surgery Consortium for Assessment and Research (NOSCAR) highlighted the challenges and limitations in implementing NOTES and set guidelines for future development and progress.
Improving Instruments
The medical device companies are racing to devise solutions for every problem we encounter in NOTES. Building on the large innovations in instruments and technology used in laparoscopic surgery (Figs. 69.1, 69.2, 69.3, and 69.4), the industry is quickly producing futuristically designed instruments to break down the barriers delaying NOTES’s progress. This rush in innovations and design has allowed a steady progress in NOTES over a shorter period of time compared to the early slow progress in the laparoscopic surgery. Enterotomy site closure is currently one of the rate-limiting steps in the race for NOTES transfer from animal models to humans. To achieve an efficient closure, we need a device that allows bimanual tissue manipulation, full-thickness tissue approximation and plication to produce a leak-proof efficient closure of the enterotomy site.
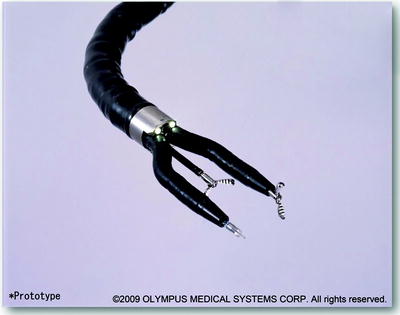
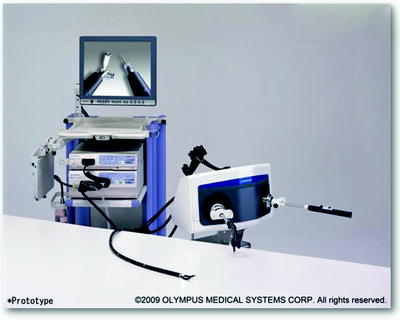

Fig. 69.1
A pulmo-NOTES prototype with two arms and an additional working channel
Fig. 69.2
A whole NOTES system with the steering unit
Fig. 69.3
Another NOTES prototype with steerable working channels is shown

Multiple closure methods and devices have been recently described and are all currently undergoing extensive testing in animal models to determine which one is the most efficient and easy to use. Methods vary from simply using endoclips to more sophisticated instruments with futuristic designs. The target at this stage in NOTES development is to produce a leak-proof closure regardless of the cost. Later on, when different closure methods produce similar results, cost will become an important issue.
Pulmo-NOTES
Thoracoscopy and mediastinoscopy are used as minimally invasive access routes to the mediastinum and pleural cavity and have proven to have clear advantages over traditional open techniques. Such endoscopic approaches allow tissue resection, sampling and staging as well as the application of microsurgical techniques like direct optical magnification of mediastinal pathology. However, the initial enthusiasm and excitement accorded to endoscopic techniques to the thorax have not taken off as fast as may have been first anticipated. The incisions even if small are painful, and the hospital stay is still relatively long, while the complications, although less common, are still significant. Furthermore, they are only applicable to potential targets limited to the outer third of the lung parenchyma.
In contrast, transoesophageal mediastinoscopy and thoracoscopy could eliminate chest wall trauma and allow medial access by using the oesophagus as the entry site into the posterior mediastinum and pleural space. The transoesophageal approach provides a direct ready access to the mediastinum and thoracic cavity allowing a direct visualisation of anatomical structures. The posterior mediastinum in particular is remote from the body surface and delimited by critical and delicate structures, such as the descending thoracic aorta, the oesophagus, the azygos vein and the autonomic ganglia and nerves.
Most diagnostic and therapeutic natural orifice transluminal endoscopic surgery procedures refer to the peritoneal cavity. Only a few experimental studies have addressed natural orifice transluminal endoscopy in other areas of the body such as the mediastinum. Concerns regarding the complications of transoesophageal mediastinoscopy, such as infection and bleeding, secure closure and healing of the oesophageal incision have limited the attempts at such studies. Furthermore, to date, it has not been ascertained whether NOTES mediastinoscopy performed with flexible endoscopes and insufflations of room air increases the risk of cardiorespiratory depression. It has been shown that manual on-demand endoscopic insufflation in the peritoneal cavity occasionally leads to respiratory compromise. Moreover, due to the closeness of critical structures such as the heart and the pleura, mediastinal NOTES might increase the risk of injury of vitally important organs.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


