In its broadest sense, myocarditis refers to any inflammation of the myocardium. Inflammation can be found after any form of injury to the heart, including ischemic damage, mechanical trauma, and genetic cardiomyopathies. More specifically, however, classic myocarditis refers to inflammation of the heart muscle occurring as a result of exposure to either discrete external antigens (such as viruses, bacteria, parasites, toxins, or drugs) or internal triggers, such as autoimmune activation against self antigens. Although viral infection remains the most commonly identified cause for myocarditis, drug hypersensitivity and toxic drug reactions, other infections, and peripartum cardiomyopathy also can lead to myocarditis.
The pathogenesis of myocarditis is a classic paradigm of cardiac injury followed by immunologic response from the host as cardiac inflammation. The relative incidence of viral causes is continually evolving as new diagnostic tools based on molecular epidemiology become available. Indeed, more than 20 viruses have been associated with myocarditis, and the most frequent are currently parvovirus B19 (PVB19) and human herpesvirus 6.1 Historically, enteroviruses such as coxsackievirus B were the most commonly identified pathogens, and strains of enterovirus remain widely used in rodent models of the disease.2,3 If the host immune response is overwhelming or inappropriate, the inflammation may destroy the heart tissue acutely or may linger on, producing cardiac remodeling that leads to dilated cardiomyopathy (DCM), heart failure, or death. Fortunately for most patients, clinical myocarditis often is self-limited if proper support and follow-up care are available. In many cases the virus is cleared successfully, and the immune response is downmodulated. In some patients, however, an autoimmune reaction to endogenous antigens lingers beyond this phase and can cause persistent cardiac dysfunction. Sometimes viral genomes persist in the heart with or without acute inflammation.4 Viral genomes commonly are detected in endomyocardial biopsy (EMB) specimens from patients with DCM and may signal a disease-related infection. As discussed in this chapter, with new insights into the understanding of pathophysiology of myocarditis and new therapies for this condition, the outlook for affected patients is continuing to improve.
Epidemiology
A comprehensive estimate of the disease burden of myocarditis should include morbidity and mortality in patients with myocarditis who present with sudden death, heart failure, and chest pain syndromes. No such integrated estimate exists, yet the contribution of myocarditis in these individual clinical scenarios has been reported. In clinical case series of sudden death, myocarditis often is the third leading cause after hypertrophic cardiomyopathy and congenital and atherosclerotic coronary artery disease.5 In autopsy studies of young adults, myocarditis is responsible for 4% to 12% of sudden deaths. This rate should be seen in the context of the unselected diagnosis rate of myocarditis, 0.11% of 377,841, in autopsies registered in Japan from 1958 to 1977. Myocarditis is responsible for a substantial minority of DCM cases (see alsoChapter 25). In a review of DCM case series from 1978 to 1995 in which EMB was performed, the incidence of biopsy-proven myocarditis in patients with DCM varied widely, ranging from 0.5% to 67%, with an average of 10.3%. Longer duration of symptoms is associated with a lower rate of active inflammation on histologic examination. Approximately 10% to 50% of nonischemic cardiomyopathy cases with symptom duration less than 6 months are due to myocarditis, a rate that varies depending on the histologic or clinical diagnostic criteria used.2 Data from the U.S. children’s cardiomyopathy registry, in which 46% (222/485) of children with an identified cause of DCM had myocarditis, are illustrative of recent reports. As in most DCM case series, only a minority of children in this series, 34% of 1426, had a specific cause for DCM identified.6
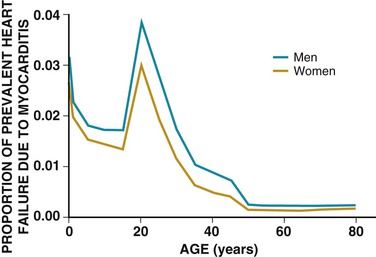
A recent analysis of hospital dismissal ICD-9 codes estimated that between 0.5% and 4% of cases of prevalent heart failure are due to myocarditis.7 This report and most case series show a slight male predominance, which may be mediated by sex hormones. The prevalence of myocarditis as a cause of cardiomyopathy is relatively high in the first year of life, declines during late childhood, and peaks in the early 20s (Fig. 67-1). This method probably underestimates the true prevalence of myocarditis, because the diagnostic test, EMB, is infrequently performed outside of referral medical centers. The primary obstacle to true population-based estimates of the incidence and prevalence of myocarditis is the lack of a sensitive and specific noninvasive diagnostic test.
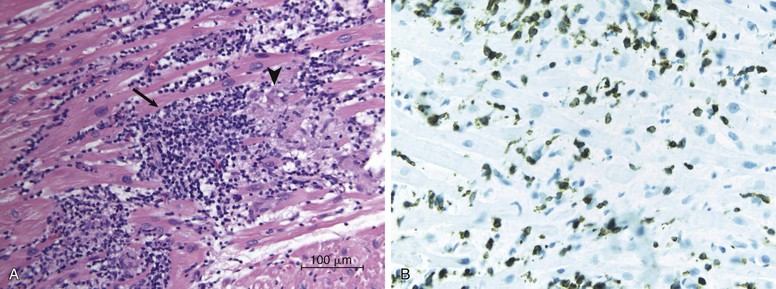
The differing histologic criteria used to define myocarditis are responsible for some of the variation in the reported prevalence of myocarditis. The standard “Dallas criteria” define idiopathic myocarditis as an inflammatory infiltrate of the myocardium with necrosis and/or degeneration of adjacent myocytes not typical of the ischemic damage associated with coronary artery disease (Fig. 67-2A; Table 67-1).8 These criteria have been criticized because of interreader variability in interpretation, lack of prognostic value, and low sensitivity due in part to sampling error. Specific immunohistochemical stains that detect cellular antigens, such as anti-CD3 (T lymphocytes), anti-CD68 (macrophages), and class I and II human leukocyte antigens (Fig. 67-2B), may have greater sensitivity for small infiltrates than that of hematoxylin-eosin. Markers of complement activity such as C4d also are commonly found in native cardiomyopathic hearts.9 Newer immunohistochemical stains have a greater predictive value for cardiovascular events than the Dallas criteria.10
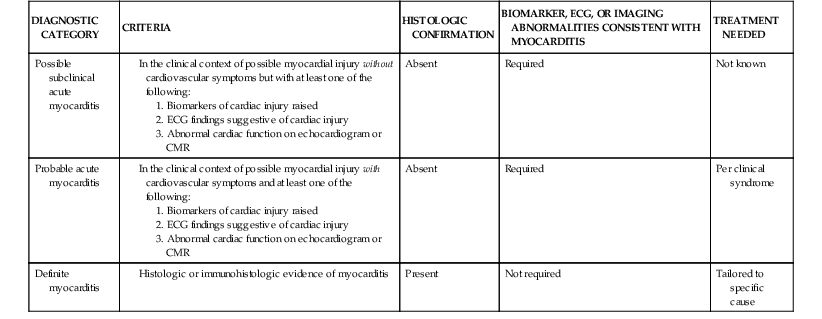
Modified from Leone O, Veinot JP, Angelini A, et al: 2011 Consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol 21:245, 2012.
The presence of viral genomes in heart tissue may indicate an active infectious myocarditis. In the post-transplantation setting, the presence of viral genomes in myocardial biopsy material predicts future rejection episodes and graft loss in children.11 Viruses commonly tested for in the setting of suspected myocarditis are PVB19, adenovirus, cytomegalovirus, enterovirus, Epstein- Barr virus, hepatitis C virus, and herpes simplex viruses 1, 2, and 6 and influenza viruses A and B. A causal relationship between PVB19 genomes in EMB tissue, particularly in low copy number, and cardiac disease has been questioned, however. New diagnostic criteria that rely on higher PVB19 copy numbers or evidence of active viral replication have been proposed.12 Although the criteria for diagnosis of infectious myocarditis are evolving, most authorities would consider a positive viral genome assay in the setting of heart failure or anginal-type chest pain without alternative explanation to indicate active viral myocarditis. For epidemiologic studies in which universal EMB is not feasible, diagnostic classifications that rely on clinical syndromes, biomarkers, and/or imaging abnormalities have been used13 (Table 67-2).
Modified from Sagar S, Liu PP, Cooper LT Jr: Myocarditis. Lancet 379:738, 2012.
Specific Etiologic Agents
In a majority of cases, myocarditis is triggered by an inciting event, such as infection or exposure to a drug or toxin, that activates the immune response. A subset of cases is due to primary immunologic abnormalities in the affected patient. Advanced techniques in virology, immunology, and molecular biology have demonstrated that there are many potential causes of myocarditis. Almost any infectious agent has been associated with myocarditis. In clinical practice, however, it is often difficult to identify a specific etiologic agent.
Viruses
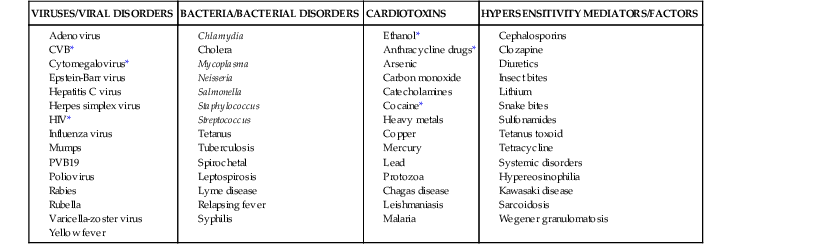
Viral infection has been implicated as one of the most common infectious causes of myocarditis (Table 67-3). The earliest evidence of virus infection and its association with myocarditis and pericarditis was acquired during outbreaks of influenza, poliomyelitis, measles, mumps, and pleurodynia associated with enterovirus infection.14 Modern virologic and molecular techniques have demonstrated that adenoviruses, enteroviruses, and parvovirus are among the most commonly identified infectious agents in myocarditis. The precise incidence of myocarditis that is caused by these agents varies geographically and temporally. Nevertheless, in meta-analyses, polymerase chain reaction (PCR) studies in patients with clinically suspected myocarditis or cardiomyopathy who subsequently underwent heart biopsy demonstrated that virus could be identified 3.8 times more frequently in patients with myocarditis than in control subjects. Additional evidence indicates that persistence of viral genome in patients with cardiomyopathy is associated with increased ventricular dysfunction and worse outcome during follow-up.15
Enterovirus Including Coxsackieviruses.
Coxsackievirus is a member of the Enterovirus genus, Picornaviridae family. It is a nonenveloped lytic virus. Its capsid proteins harbor a single-strand, positive-strand RNA genome of 7.4 Kb. Throughout the history of studies that address the causes of myocarditis, enteroviruses such as coxsackievirus B3 or echovirus are commonly identified in a subset of patients at a higher frequency than in control subjects. Using molecular techniques such as PCR and in situ hybridization, enterovirus genome has been identified in the heart of 15% to 30% of patients with myocarditis and 7% to 30% of specimens with DCM, although the incidence in different studies varies considerably.15 Coxsackievirus infection meets the criteria of Koch’s postulates as a cause of myocarditis in humans: It can be regularly found in the lesions of the disease; it has been isolated in pure culture from patients with myocarditis; and when inoculated into a mouse it can recapitulate the disease, after which the virus can be recovered from the heart of the infected mouse.
Coxsackievirus is a close relative of poliovirus and rhinovirus, viruses that have been studied extensively. Although the disease phenotypes are very different, the many similarities in viral replication cycles have facilitated understanding of the mechanisms by which coxsackievirus can cause disease. Coxsackievirus typically enters the host through the gastrointestinal or respiratory system. It uses the coxsackievirus-adenovirus receptor (CAR), a transmembrane adhesion protein, as its primary receptor for cell entry. It can cause a broad range of clinical syndromes including meningitis, skin rashes, acute respiratory illness, skeletal myositis, and myocarditis.
Most recently, evaluation of patients with myocarditis has demonstrated a decrease in the prevalence of enteroviruses in the myocardium. This is particularly evident in western Europe. The reason for this decrease is not clear, but it may be related to a herd immunity that occurs after a period of prolonged exposure to the virus. The lower incidence also may be confounded by seasonal outbreaks of enterovirus infections, thereby making the exact incidence dependent on the outbreaks.
Adenovirus.
Adenoviruses are nonenveloped DNA viruses that also use CAR (adenovirus types 2 and 5), as well as integrins, as receptors for entry into the target cell. The adenovirus capsid harbors a double-stranded DNA genome. Adenoviruses commonly infect mucosal surfaces. Adenovirus genome is consistently identified in a subset of patients with myocarditis. The incidence in myocarditis patients has been recorded to be as high as 23% but as low as less than 2%.15 Although mechanisms of adenoviral infection have been studied in considerable detail in cell culture and other diseases, it has been challenging to study adenovirus-mediated myocarditis, in the face of difficulties identifying an appropriate mouse model using the same adenoviruses that affect humans.
Parvovirus.
Recently, considerable attention has focused on the role of PVB19 in the pathogenesis of myocarditis because of the high prevalence of PVB19 DNA in hearts of patients with myocarditis. Parvovirus is a nonenveloped, nonlytic virus with a single-strand, positive-strand DNA genome of approximately 5.6 kb. Humans are the only known host for PVB19, making it challenging to study in animal models, but examples of myocarditis in mice stimulated with the capsid protein VP1 or antibodies against VP1 have been reported.15 Its primary receptor is globoside, also known as group P antigen. This antigen is found primarily on erythroid progenitors, erythroblasts, and megakaryocytes. It also has been shown to be expressed on endothelial cells. This finding may be important for its role in the pathogenesis of myocarditis. The infection is thought generally to be spread by the respiratory route. The incidence of infection in the general population is very high, with evidence of PVB19 infection demonstrated in approximately 50% of children at age 15, and detectable IgG directed against PVB19 found in as many as 80% of elderly patients.15 Using PCR studies, PVB genome has been identified in 11% to 56% of patients with myocarditis and in 10% to 51% of patients with DCM.
In keeping with the high prevalence of PVB19 in the general population, the pathogenic role of PVB19 continues to be clarified. In one study, PVB19 was assessed by immunohistochemistry and PCR assay. The investigators found that PVB19 was detectable by immunohistologic analysis in 65% of patients with myocarditis, 35% of patients with DCM, and 8% of noninflamed control hearts. Viral load was then assessed by genome copy numbers in the samples that were positive for PVB19 on immunohistologic analysis. Viral load was significantly higher in patients with acute myocarditis, followed by those with DCM, and lowest in the patients with normal hearts without inflammation.12 In addition, viral RNA replicative intermediates were detected only in patients with inflamed hearts. These findings indicate that the amount of PVB19 viral DNA is associated with the disease phenotype. Of importance, the virus was found in endothelial cells and not myocardial cells. Other studies have suggested a bystander role for PVB19 in adult myocarditis,16 with persistence of low-level PVB19 titers a frequent finding, but unrelated to ongoing myocardial injury. Additional experimentation is needed to determine mechanisms by which PVB19 could contribute to myocarditis and cardiomyopathy.
Human Immunodeficiency Virus.
The improved survival of patients with human immunodeficiency virus (HIV) infection (see alsoChapter 70) has increased the incidence of heart disease in this population, but part of that increase reflects a higher incidence of coronary artery disease. In retrospective series and autopsy studies in patients infected with HIV, the incidence of cardiac involvement ranged from 25% to 75%. Clinical cardiovascular presentations associated with HIV infection include myocarditis, pericarditis, DCM, arrhythmias, and vascular diseases. Myocarditis with lymphocytic infiltration has been reported to be present in 40% to 52% of patients who die of AIDS. The incidence of cardiac disease, however, appears to have decreased with increased antiretroviral therapy. This is especially true as it relates to DCM, pericardial disease, and arrhythmias. The incidence of cardiomyopathy, myocarditis, and pericardial diseases correlates with the severity of the HIV infection as measured by low CD4+ count or high viral titers. Owing to ongoing changes in therapy for HIV infection, the exact incidence of myocardial diseases is not clear, but it continues to be a problem. In addition, many patients in developing regions of the world do not received highly active antiretroviral therapy and may present with cardiac disease. Although it is clear that HIV infection can be associated with ventricular dysfunction, the mechanisms by which this occurs have not been fully elucidated;. however, activation of cytokines and alteration of immune cells that affect cardiac function are likely to be involved. Convincing evidence that HIV directly infects the myocardium is lacking. The pathogenesis of HIV-associated cardiomyopathy is complicated by infection with pathogens that are associated with immunosuppression, malnutrition, and other confounding effects.
Hepatitis C Virus.
Hepatitis C virus infection appears to be mainly associated with cardiomyopathy in Asian countries such as Japan. A low incidence of hepatitis C virus antibodies (4.4%) was identified in patients who were studied in the Myocarditis Treatment Trial. This occurrence rate was nevertheless higher than that (1.8%) in the general U.S. population. Perhaps the higher incidence of hepatitis C virus infection in DCM is related to the overall higher incidence of this infection in Asia. Myocardial biopsy samples from patients with cardiomyopathy have demonstrated the presence of the hepatitis C viral genome, and a rise in serum antibody titers has been documented in patients so affected. The phenotype associated with hepatitis C virus also has been reported to include hypertrophic cardiomyopathy, suggesting that hepatitis C may have a direct effect on growth and hypertrophy of the myocardial cells. Symptomatic myocarditis generally is observed in the first to third weeks of illness. It has been reported that heart function can return to normal with clearance of the virus.
Influenza Virus.
Influenza A virus infection is a well-recognized cause of myocarditis, and this association should be kept in mind during periodic outbreaks of influenza A. The exact incidence of myocarditis with influenza A outbreaks is not known, but it generally is considered to be in the 5% range. During pandemics such as the 2009 H1N1 pandemic, myocarditis has been reported in up to 5% to 15% of cases as diagnosed by changes on the electrocardiogram (ECG) and presence of cardiac symptoms. Some cases manifested with fulminant myocarditis. Histopathologic examination usually demonstrates presence of the inflammatory infiltrate that is typical of myocarditis.17
Modified from Elamm C, Fairweather D, Cooper LT: Pathogenesis and diagnosis of myocarditis. Heart J 98:835, 2012.
Bacteria
Nonviral pathogens such as bacteria and parasites can affect the heart and in some cases, activate an immune reaction in the heart. Virtually any bacterial agent can cause myocardial dysfunction, but it does not necessarily mean that the bacterium has infected the myocardium. In the case of sepsis or other severe bacterial infection, the myocardial dysfunction generally is attributed to activation of inflammatory mediators (seeChapter 22). Of note, however, bloodstream infection by virtually any bacterial infection can result in metastatic foci in the myocardium. This finding is most commonly associated with bacterial endocarditis. Some bacterial infections are well known to have specific effects on the heart that can be mediated by direct infection or activation of inflammatory mechanisms. The most common of these include diphtheria, rheumatic heart disease, and streptococcal infections.
Corynebacterium Infection.
Myocardial involvement with Corynebacterium diphtheriae is a serious complication and is the most common cause of death in diphtheria. In up to one half of fatal cases, evidence of cardiac involvement can be found. Studies from the last decade indicate that there is evidence of myocardial involvement in 22% to 28% of patients. The overall incidence has decreased in developed countries because of vaccination, but recently, there is a growing number of unprotected individuals in developed countries as well. This may be related to vaccine avoidance. C. diphtheriae produces an exotoxin that severely damages the myocardium and the cardiac conduction system. Cardiac damage is due to the liberation of this exotoxin that inhibits protein synthesis by interfering host translational mechanisms. The toxin appears to have a particular affinity for the cardiac conduction system. Both antitoxin therapy and antibiotics are important in the treatment of diphtheria.
Streptococcal Infection.
The most commonly detected cardiac complication after beta-hemolytic streptococcal infection is acute rheumatic fever that is followed by rheumatic valve disease in approximately 60% of patients.18,19 Rarely, involvement of the heart by the streptococcus may produce a nonrheumatic myocarditis distinct from acute rheumatic carditis.20 This clinical entity is characterized by presence of an interstitial infiltrate composed of mononuclear cells with occasional polymorphonuclear leukocytes, which may be focal or diffuse. In contrast with rheumatic heart disease, streptococcal myocarditis usually occurs coincident with the acute infection or within a few days of the pharyngitis. Electrocardiographic abnormalities, including ST elevation and prolongation of the PR and QT intervals, are common.20,21 Rare sequelae may include sudden death, conduction disturbances, and arrhythmias.
Tuberculosis.
Involvement of the myocardium by Mycobacterium tuberculosis (not tuberculous pericarditis) is rare. Tuberculous involvement of the myocardium occurs by means of hematogenous or lymphatic spread or may arise directly from contiguous structures and may cause nodular, miliary, or diffuse infiltrative disease. On occasion, it may lead to arrhythmias including atrial fibrillation and ventricular tachycardia, complete atrioventricular block, heart failure, left ventricular aneurysms, and sudden death.22
Whipple Disease.
Although overt involvement is rare, intestinal lipodystrophy, or Whipple disease, is not uncommonly associated with cardiac involvement. Periodic acid–Schiff–positive macrophages can be found in the myocardium, pericardium, coronary arteries, and heart valves of patients with this disorder. Electron microscopy has demonstrated rod-shaped structures in the myocardium similar to those found in the small intestine, representing the causative agent of the disease, Tropheryma whipplei, a gram-negative bacillus related to the actinomycetes. An inflammatory infiltrate and foci of fibrosis also may be present. The valvular fibrosis may be severe enough to result in aortic regurgitation and mitral stenosis. Although it usually is asymptomatic, nonspecific electrocardiographic changes are most common; systolic murmurs, pericarditis, complete heart block, and even overt congestive heart failure may occur. Antibiotic therapy appears to be effective in treatment of the basic disease, but relapses can occur, often more than 2 years after initial diagnosis.
Lyme Carditis.
Lyme disease is caused by a tick-borne spirochete (Borrelia burgdorferi). It usually begins during the summer months with a characteristic rash (erythema chronicum migrans), followed by acute neurologic, joint, or cardiac involvement, usually with few long-term sequelae. Early studies indicated that up to 10% of untreated patients with Lyme disease demonstrated evidence of transient cardiac involvement, the most common manifestation being atrioventricular block of variable degree. With the early use of antibiotics, however, Lyme carditis is now considered to be a rare manifestation.23 Syncope due to complete heart block is frequent with cardiac involvement because of the commonly associated depression of ventricular escape rhythms. Diffuse ST-segment and T wave abnormalities are transient and usually asymptomatic. An abnormal gallium scan is compatible with cardiac involvement, and the demonstration of spirochetes in myocardial biopsy specimens of patients with Lyme carditis suggests a direct cardiac effect. Patients with second-degree or complete heart block should be hospitalized and undergo continuous electrocardiographic monitoring. Temporary transvenous pacing may be required for a week or longer in patients with high-grade block. It is thought that antibiotics can prevent subsequent complications and may shorten the duration of the disease; therefore they are used routinely in patients with Lyme carditis. Intravenous antibiotics are suggested, although oral antibiotics can be used when only mild cardiac involvement is present. Corticosteroids may reduce myocardial inflammation and edema, which in turn can shorten the duration of heart block. It is thought that treatment of the early manifestations of the disease will prevent development of late complications.
Protozoa
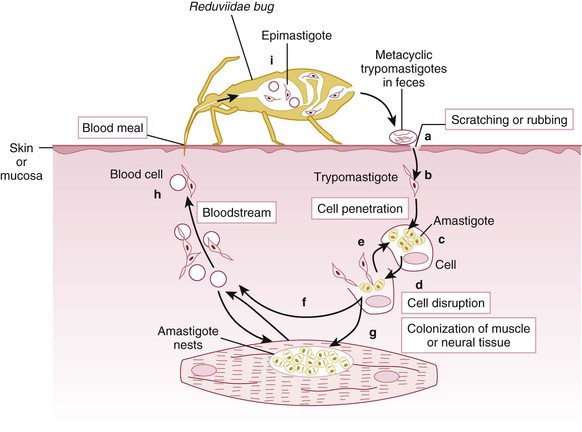
Chagas disease is one of the major causes of nonischemic cardiomyopathy throughout the world, although the incidence is changing. In a remarkable tale of discovery at the beginning of the 20th century, Carlos Chagas almost single-handedly identified the parasite, Trypanosoma cruzi (T. cruzi), that causes the entity now known as Chagas disease. He also elucidated the relatively complex life cycle of the parasite in poor, rural areas of Brazil.24 The parasite resides in an infected host such as an armadillo or a domestic cat, wherein the parasite replicates. The parasite then infects triatomine insects, including the hematophagous reduviid bug that feeds on the blood of infected vertebrate carriers. The triatomine acts as the vector of infection when it bites a human, depositing the parasite in its feces in the area of the bite wound, conjunctiva, or other mucous membranes. Once within the now-infected individual, the parasite replicates and infects target organs such as the heart. Parasitic infection of cardiac myocytes and activation of the associated immune function damage the heart and other organs lead to the clinical manifestations of Chagas disease (see Fig. 67-3 for life cycle).25
Chagas disease is endemic in poor, rural areas of Central and South America (see Fig. e67-1). The distribution of Chagas disease is changing to include more urban and traditionally non-endemic areas because of migration of infected individuals from the rural to urban areas. Vector control initiatives in the endemic areas and aggressive screening of the blood supply has reduced the overall incidence of Chagas disease. In the 1980s, 17.4 million people were infected in 18 endemic countries.26 By 2005, it was estimated that the number of infected persons had dropped to nearly 7.7 million. In 1990, it was estimated that 700,000 new cases were diagnosed each year. In 2006, that number had decreased to 41,200. Similarly, the number of annual deaths from Chagas disease has decreased, from 50,000/year in 1990 to approximately 12,500/year.25 However, at the same time that Chagas disease is decreasing worldwide, the incidence in the developed world is increasing because of immigration from endemic areas. It is currently estimated that approximately 300,000 people in the United States are infected with T. cruzi.25 This has important implications in relation to blood transfusion and organ donation, because the infectious agent can be transferred from donor to recipient—a particularly important consideration in the immunocompromised transplant recipient.
Symptoms from T. cruzi infection typically begin 1 to 2 weeks after a bite from an infected triatomine or can occur up to a few months after transfusion of infected blood. The parasite load can affect the severity of clinical presentation. The acute phase is accompanied by the presence of parasites in the blood smear. The acute phase of T. cruzi infection lasts for 4 to 8 weeks. During the acute phase of parasite infection, most affected patients are either asymptomatic or have a mild, subacute febrile illness. Other potential manifestations include adenopathy, hepatomegaly, myocarditis, and meningoencephalitis. Cardiovascular abnormalities during the acute phase might include nonspecific ECG changes, first-degree atrioventricular block, and cardiomegaly on chest x-ray examination. Death occurs from myocarditis or meningoencephalitis in less than 5% to 10% of symptomatic patients. In up to 90% of patients, the symptoms of disease resolve spontaneously. Of these, approximately 60% to 70% never develop chronic Chagas disease manifestations even in the absence of treatment with trypanocidal drugs, but these patients will remain seropositive throughout life. Aside from seropositivity for T. cruzi, the patients without manifestations of disease exhibit no signs or laboratory findings of Chagas disease, as described further on. The other 30% to 40% of patients ultimately develop more typical manifestations of the chronic form of Chagas disease. Treatment with antiparasite drugs such as benznidazole usually can cure the patient during the acute illness.24,25 The chronic phase of T. cruzi
Only gold members can continue reading. Log In or Register to continue

 ). The distribution of Chagas disease is changing to include more urban and traditionally non-endemic areas because of migration of infected individuals from the rural to urban areas. Vector control initiatives in the endemic areas and aggressive screening of the blood supply has reduced the overall incidence of Chagas disease. In the 1980s, 17.4 million people were infected in 18 endemic countries.26 By 2005, it was estimated that the number of infected persons had dropped to nearly 7.7 million. In 1990, it was estimated that 700,000 new cases were diagnosed each year. In 2006, that number had decreased to 41,200. Similarly, the number of annual deaths from Chagas disease has decreased, from 50,000/year in 1990 to approximately 12,500/year.25 However, at the same time that Chagas disease is decreasing worldwide, the incidence in the developed world is increasing because of immigration from endemic areas. It is currently estimated that approximately 300,000 people in the United States are infected with T. cruzi.25 This has important implications in relation to blood transfusion and organ donation, because the infectious agent can be transferred from donor to recipient—a particularly important consideration in the immunocompromised transplant recipient.
). The distribution of Chagas disease is changing to include more urban and traditionally non-endemic areas because of migration of infected individuals from the rural to urban areas. Vector control initiatives in the endemic areas and aggressive screening of the blood supply has reduced the overall incidence of Chagas disease. In the 1980s, 17.4 million people were infected in 18 endemic countries.26 By 2005, it was estimated that the number of infected persons had dropped to nearly 7.7 million. In 1990, it was estimated that 700,000 new cases were diagnosed each year. In 2006, that number had decreased to 41,200. Similarly, the number of annual deaths from Chagas disease has decreased, from 50,000/year in 1990 to approximately 12,500/year.25 However, at the same time that Chagas disease is decreasing worldwide, the incidence in the developed world is increasing because of immigration from endemic areas. It is currently estimated that approximately 300,000 people in the United States are infected with T. cruzi.25 This has important implications in relation to blood transfusion and organ donation, because the infectious agent can be transferred from donor to recipient—a particularly important consideration in the immunocompromised transplant recipient.