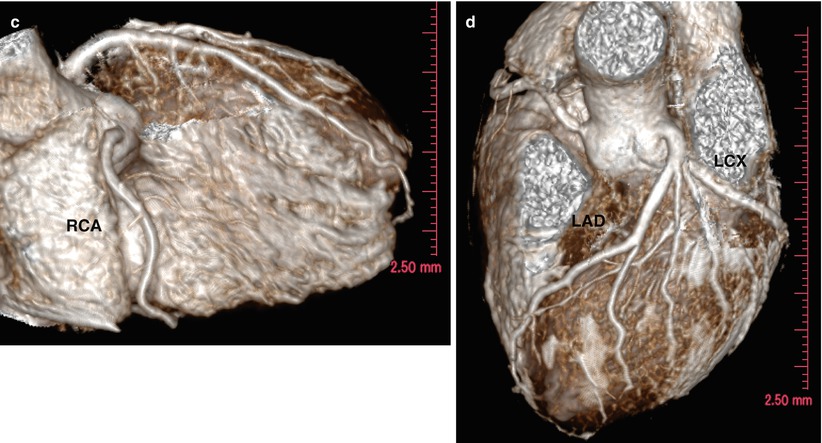
Fig. 7.1
1.5 T Free-breathing whole heart coronary MR angiography in a subject with normal coronary artery. Non-contrast-enhanced three-dimensional coronary MR angiography images were acquired with a 1.5 T MR imager by using a steady-state free precession (SSFP) sequence, navigator echo gating, T2 preparation, spectral presaturation inversion-recovery fat saturation (repetition time/echo time, 4.6/2.3 ms; flip angle, 90°; sensitivity encoding [SENSE] factor, four; field of view, 280 × 280 × 120 mm; acquisition matrices, 256 × 256 × 80; reconstruction matrices, 512 × 512 × 160). (a) Thin-section maximal intensity projection (MIP) images of right coronary artery (RCA). (b) Thin-section MIP images of left main and let anterior descending arteries (LAD). (c) Volume rendered images of RCA. (d) Volume rendered images of LAD and left circumflex coronary artery (LCX)
Learning Point
Coronary MR angiography allows noninvasive visualization of the coronary artery without exposing the patients to ionizing radiation.
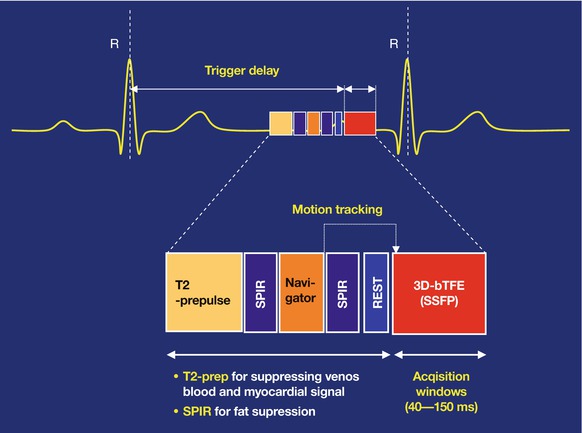
Fig. 7.2
Schematic representation of pulse sequence of free-breathing 1.5 T coronary MR angiography. Image acquisition is performed after a trigger delay from the R wave of the ECG. The imaging block is preceded by a T2 preparation, spectral presaturation inversion-recovery fat saturation, and a navigator pulse for respiratory motion compensation. These sequence blocks are repeated with every heart cycle
Learning Point
At 1.5 T, excellent blood contrast can be obtained by using SSFP MR angiographic sequence without injection of gadolinium-based contrast medium.
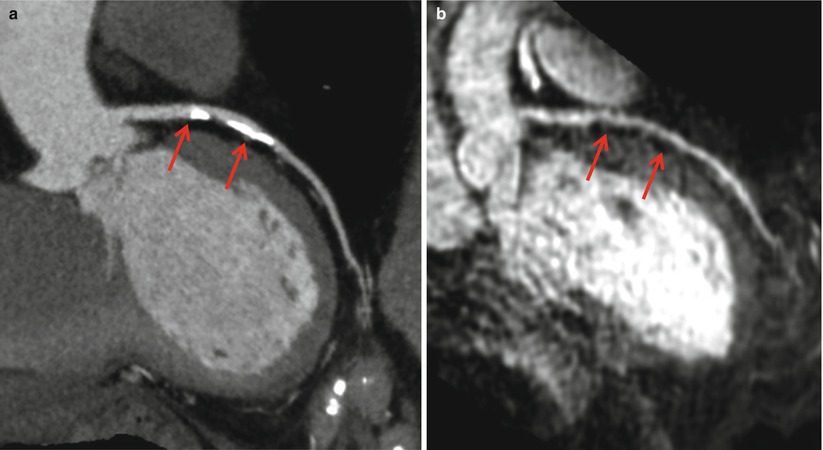
Fig. 7.3
Comparison of coronary CT angiography and MR angiography in a patient with calcified plaque at LAD. A 64-year-old female patient with chest pain. Non-contrast-enhanced three-dimensional coronary MR angiography images were acquired with a 1.5 T MR imager by using a steady-state free precession (SSFP) sequence, navigator echo gating, T2 preparation, spectral presaturation inversion-recovery fat saturation (repetition time/echo time, 4.6/2.3 ms; flip angle, 90°; sensitivity encoding [SENSE] factor, four; field of view, 280 × 280 × 120 mm; acquisition matrices, 256 × 256 × 80; reconstruction matrices, 512 × 512 × 160). (a) Curved multi-planar reconstruction (MPR) images of coronary computed tomography (CT) images showed diffuse calcified plaque (arrows) in the proximal LAD. (b) Thin-section MIP image of coronary MR angiography revealed patent LAD (arrows)
Learning Point
Coronary MR angiography may provide better diagnostic accuracy in patients with heavily calcified plaque.
7.1.3 Image Analysis
CMRA can be assessed on source 3D images, multiplanar reformation (MPR) images, thin maximal intensity projection (MIP) images, or volume-rendered images.
The presence or absence of significant coronary stenosis on CMRA is qualitatively assessed.
The current whole-heart CMRA approach could not provide sufficient spatial resolution for quantitative analysis of luminal diameter narrowing of the coronary artery.
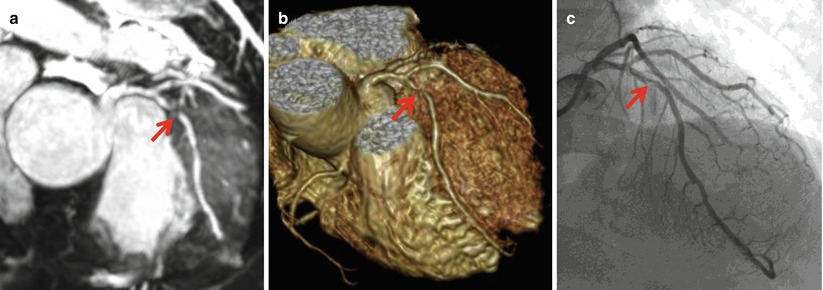
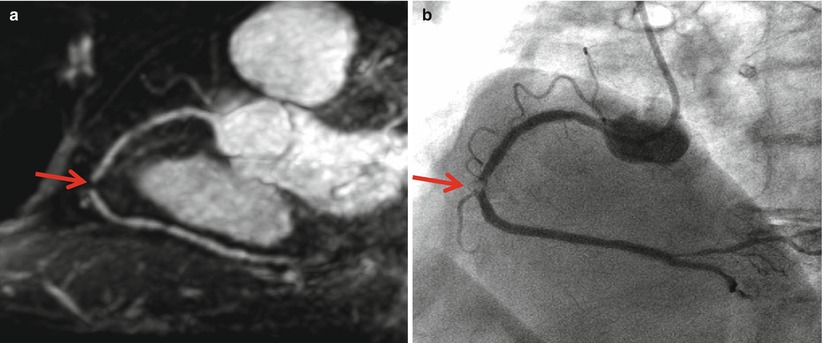
Fig. 7.4
Significant stenosis of LAD. A 65-year-old male patients with chest pain. Non-contrast-enhanced three-dimensional coronary MR angiography images were acquired with a 1.5 T MR imager by using a steady-state free precession (SSFP) sequence, navigator echo gating, T2 preparation, spectral presaturation inversion-recovery fat saturation (repetition time/echo time, 4.6/2.3 ms; flip angle, 90°; sensitivity encoding [SENSE] factor, four; field of view, 280 × 280 × 120 mm; acquisition matrices, 256 × 256 × 80; reconstruction matrices, 512 × 512 × 160). (a) Thin-section MIP and (b) volume rendered image of whole-heart coronary MR angiography showed significant stenosis of mid LAD (arrow). (c) Good agreement was observed between coronary MR angiography (arrow) and invasive coronary angiography (arrow)
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


