Mixed Germ Cell Tumors
Borislav A. Alexiev, M.D.
Allen P. Burke, M.D.
Background
Mixed germ cell tumors (GCT) are composed of more than one type of GCT element and are malignant.1 Virtually any combination of elements may be present; common combinations include teratoma, embryonal carcinoma, and yolk sac tumor, with or without seminoma. The presence of syncytiotrophoblasts with seminoma in the absence of other tumor types does not define a mixed GCT. However, other than with pure seminoma, the presence of syncytiotrophoblasts always indicates the presence of mixed elements.
Incidence and Clinical
In children, mixed GCTs account for about 20% of mediastinum GCTs, and yolk sac tumor with mature or immature teratoma is the characteristic constellation. Among children <8 years of age, some authors report a preponderance of females, while virtually all adolescent patients >8 years with mixed GCTs are males.2,3,4 After the onset of puberty, mixed GCTs can be associated with Klinefelter syndrome.5,6
In adults, mixed GCTs account for 13% to 25% of all mediastinal GCTs, second only to teratomas (40% to 60%).7,8,9,10,11,12 Virtually all adult patients are male. Most patients present with general and local symptoms identical to those in other mediastinal GCT: chest pain, cough, dyspnea, hoarseness, superior vena cava syndrome, and cardiac tamponade.12 Most cases (˜90%) show elevated serum tumor marker levels.13 Raised AFP (˜80%) is strongly correlated with a yolk sac tumor component, although teratomatous hepatoid cells and teratomatous neuroepithelium can also produce small amounts of AFP.1 Increased beta-hCG (˜30%) levels occur in mixed GCTs with a choriocarcinoma component or with syncytiotrophoblast cells.14
Gross Pathology
The tumors are often poorly circumscribed or frankly infiltrative, and show a variegated cut surface because of their different components. Cystic spaces usually indicate presence of a teratomatous component. Foci of hemorrhage and necrosis are common.
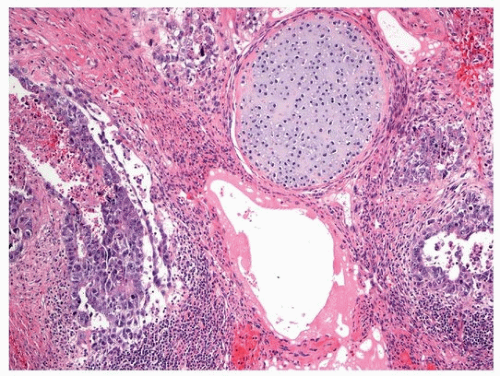 FIGURE 125.1 ▲ Mediastinal mixed GCT. Note teratoma and embryonal carcinoma components. |
Microscopic Pathology
The various types of germ cell can occur in any combination, and their appearances are identical to those occurring in pure form (Fig. 125.1). The most common mixtures in adult mediastinal mixed GCTs are teratoma + seminoma, yolk sac tumor, or embryonal carcinoma, embryonal carcinoma + seminoma, yolk sac tumor + seminoma, embryonal carcinoma + seminoma, and embryonal carcinoma + choriocarcinoma.8,15 In children, various combinations have been reported, including yolk sac tumor + embryonal carcinoma, yolk sac tumor + embryonal carcinoma + choriocarcinoma, yolk sac tumor + embryonal carcinoma + seminoma, yolk sac tumor + embryonal carcinoma + teratoma, yolk sac tumor + teratoma, and embryonal carcinoma + seminoma.3 The diagnosis should be complemented by listing each component and its approximate proportion.
The histology of metastases usually reflects the histology of the primary GCTs or one of its components; however, other germ cell components and somatic-type malignancies may occur, particularly after chemotherapy.16 Radiation and chemotherapy may produce the necrosis with inflammatory response, including xanthogranuloma, stromal fibrosis with cellular atypia, and cystic changes. Viable tumor may show loss of marker production (negative staining for AFP or hCG).1
Evaluation of Posttreatment Specimens
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


