and K. M. John Chan
(1)
Department of Cardiothoracic Surgery Hammersmith Hospital, Imperial College Healthcare NHS Trust, London, UK
Introduction
In Western developed countries, mitral valve surgery usually involves degenerative or Barlow’s valve disease, causing mitral regurgitation; the mitral valve can usually be repaired successfully. However, in developing countries, rheumatic mitral valve disease, causing mitral stenosis or regurgitation or both, is still common and repairing these valves can be more challenging.
Pre operative transoesophageal assessment of the mitral valve is essential. This is usually performed after the induction of anaesthesia and before the commencement of cardiopulmonary bypass. In most cases, this would confirm the findings of transthoracic echo, but new changes may sometimes be identified.
Setup
Optimal setup is very important in mitral valve surgery to maximise exposure and visualisation of the mitral valve. The pericardium should be lifted up on the right side and left free on the left side. This has the effect of rotating the heart upwards and towards the left, bringing the mitral valve into view when the left atrium is opened. A Cosgrove mitral retractor is used. Further visualisation of the mitral valve is enabled by incising the pericardium on top of the SVC and perpendicular to it. This allows retraction of the heart upwards when the retractors are placed.
The aorta, SVC and IVC are cannulated. An antegrade cardioplegia and a retrograde cardioplegia cannula are inserted. Tapes may be passed around the SVC and IVC. Cardiopulmonary bypass is commenced. A cross-clamp is applied. Cardioplegia is delivered antegradely to start with and then every 20 min retrogradely through a self-inflating balloon catheter while suction is applied to the aortic root.
Excision of Left Atrial Appendage
If the patient is in atrial fibrillation and ablation surgery is contemplated, the left atrial appendage is excised at this stage. The heart is lifted up, exposing the left atrial appendage. This is excised with scissors. It is then oversewn with 4/0 prolene leaving 5–10 mm above the base of the left atrial appendage. Other methods have also been used, such as stapling the left atrial appendage, ligating it from outside, either with a simple silk tie or by placing a purse string suture, or ligating it from inside by placing a purse string around its base and tightening this. However, these other methods have a higher failure rate compared to excision and suture.
Another important step, especially if ablation surgery is to be performed, is to separate out the back of the heart at the oblique sinus from the oesophagus to minimise trauma to it from the energy waves. While the heart is lifted up with the left hand, the fingers of the right hand are placed onto the back of the heart at the oblique sinus to separate it from the oesophagus. This space will fill with blood or water, thus, forming an insulating layer.
Exposing the Mitral Valve
The venous cannulation lines are placed over on the left side, supported by the mitral retractor.
Left Atriotomy
Our preferred approach to the mitral valve is through a left atriotomy. An incision is made midway between the inter-atrial septum and the origin of the right superior pulmonary vein and extended inferiorly along the left atrium towards the left inferior pulmonary vein, ending a few millimetres inferior to it. The incision is then extended superiorly a few millimetres beyond the end of the right superior pulmonary vein onto the roof of the left atrium. This incision is facilitated by the previous dissection on the SVC. Two small mitral retractors are then inserted and lifted up together, opening up the left atrium and exposing the mitral valve.
We have found that this approach to the mitral valve, together with the steps described earlier which free up the heart and allow its rotation, provides excellent exposure to the mitral valve. To improve visualisation of the mitral valve further, the incision can be extended superiorly and medially underneath the SVC and onto the roof of the left atrium.
Transseptal Approach
If surgery to the right side of the heart is also to be performed, e.g. to the tricuspid valve, the transseptal approach can be used. A vertical incision is made in the right atrium from the right atrial appendage to the inter-atrial septum. The septum is then incised at the foramen ovale.
Alternatively, an incision is made in the right atrium parallel to the inter-atrial groove about 2 cm above it. The incision is extended superiorly to the junction with the left atrium. The septum is then incised horizontally at the lower edge of the foramen ovale. It is extended superiorly to join the right atrial incision, continuing onto the roof of the left atrium. The retractor is then placed on the septum or a stay suture is applied to expose the mitral valve.
Assessing the Mitral Valve
A systematic analysis of the mitral valve is performed. The mitral valve is first inspected. Note is made of any excessive leaflet tissue, leaflet perforations, ruptured chordae or ruptured papillary muscles. The lesion is then determined using a pair of nerve hooks (Fig. 5.1). A reference point, such as P1 or the commissures, is chosen. Each part of the mitral valve leaflet is lifted up in turn and compared to the reference point to determine if there is leaflet prolapse or restriction. A variety of techniques can be used to repair the mitral valve, depending on the lesion.
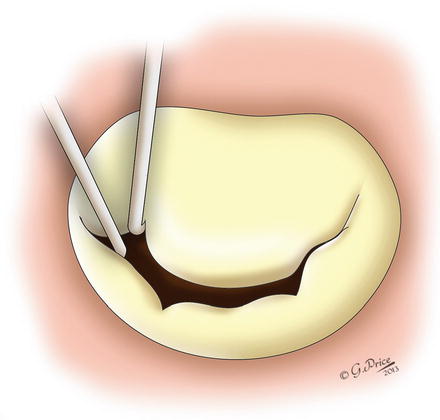
Figure 5.1
Assessing the mitral valve using a pair of nerve hooks (Printed with permission © Gemma Price)
Posterior Leaflet Prolapse
Prolapse of the posterior leaflet and, in particular, P2 prolapse is most easily repaired (Fig. 5.2). It may be due to excessive leaflet tissue as in Barlow’s disease, chordal or papillary muscle rupture or both. The aim of the repair is to restore the surface of coaptation with the anterior leaflet. This is usually achieved by excision of the prolapsing posterior leaflet.
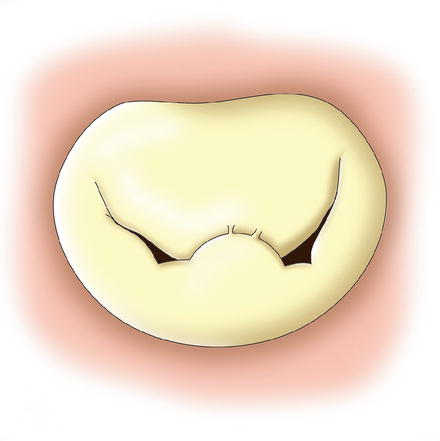




Figure 5.2
Prolapse of P2 due to ruptured chordae (Printed with permission © Gemma Price)
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
