2 Mitral Valve Diseases
Introduction: The Role of Intraoperative Transesophageal Echocardiography In Mitral Valve Surgery
Key Points
When used in that fashion, intraoperative TEE has been shown to improve outcome.
Indications
The 2003 ACC/AHA/ASE (American College of Cardiology/American Heart Association/American Society of Echocardiography) Guideline Update for the Clinical Application of Echocardiography lists the various indications for TEE.1 Several of them apply specifically to the MV and they are listed in Table 2-1.
TABLE 2-1 INDICATIONS FOR MITRAL VALVE ASSESSMENT BY TRANSESOPHAGEAL ECHOCARDIOGRAPHY
| Class I | |
| Conditions for which there is evidence for and/or general agreement that a procedure be performed or a treatment is of benefit. | |
| Class IIa | • Surgery in patients at high risk of myocardial ischemia/infarction or hemodynamic disturbances (often includes ischemic MR) |
| Conditions for which there is a divergence of evidence and/or opinion about the treatment. Weight of evidence/opinion is in favor of usefulness or efficacy. | |
| Class IIb | |
| Conditions for which there is a divergence of evidence and/or opinion about the treatment. Usefulness/efficacy is less well established by evidence or opinion. |
LA, left atrium; LA, left atrial; MR, mitral regurgitation.
From the 2003 ACC/AHA/ASE Guideline Update for the Clinical Application of Echocardiography.
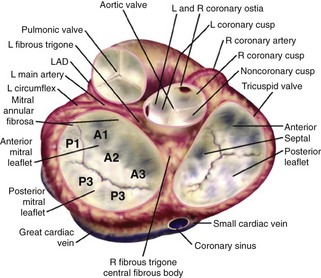
Mitral Valve Anatomy (Figure 2-1)
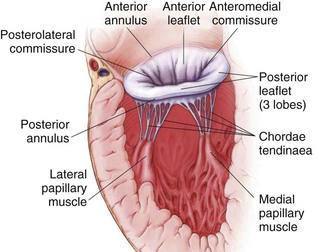
Figure 2-1 MV anatomy.
Adapted from Otto CM. Evaluation and management of chronic mitral regurgitation. N Engl J Med. 2001;345:740-746. Reproduced with permission.
Mitral Valve Nomenclature
Systematic Examination of the Mitral Valve
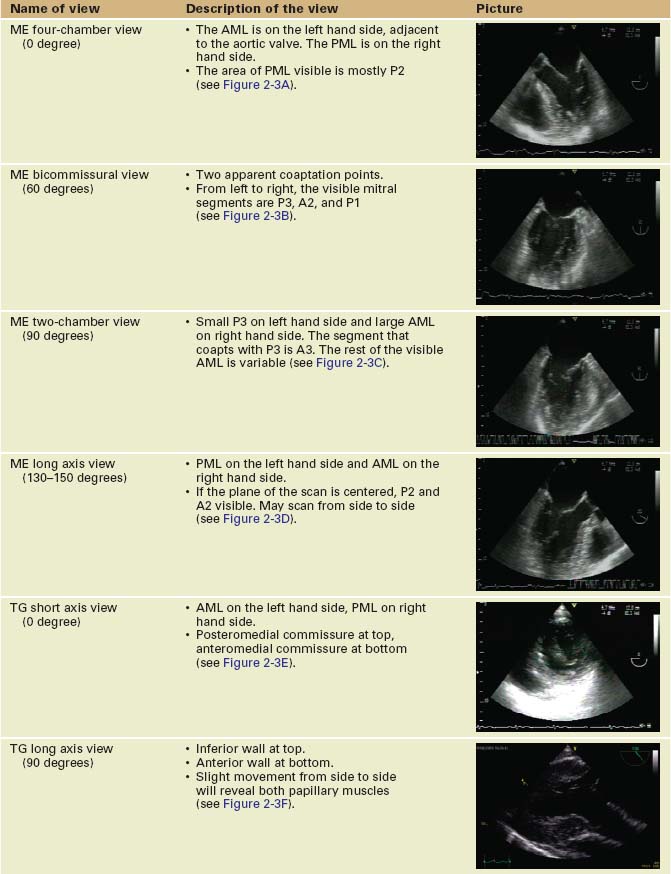
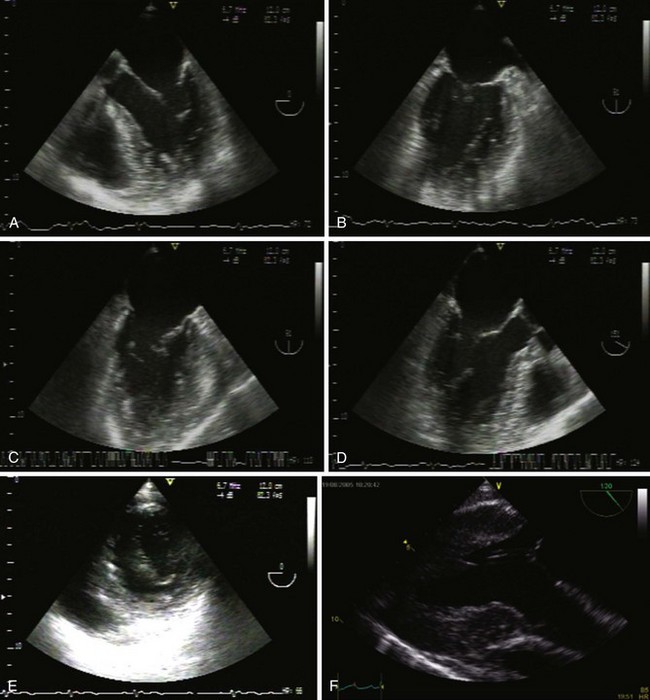
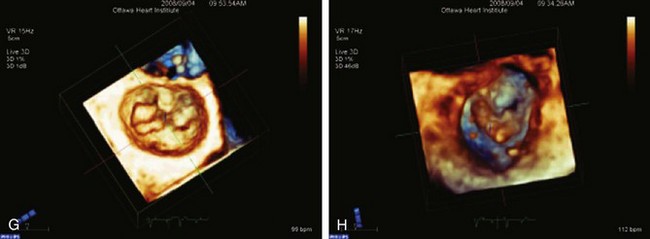
Sequence of Views (Table 2-2 and Figure 2-3)
TABLE 2-2 The Systematic Mitral Valve Examination
Key Points
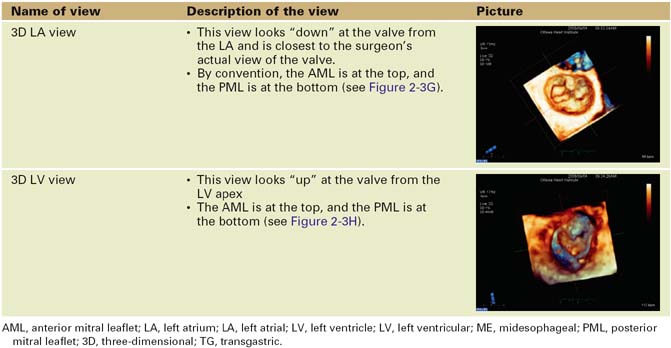
Three-Dimensional Echocardiography
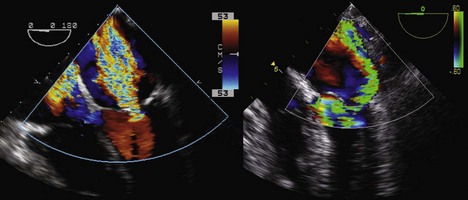
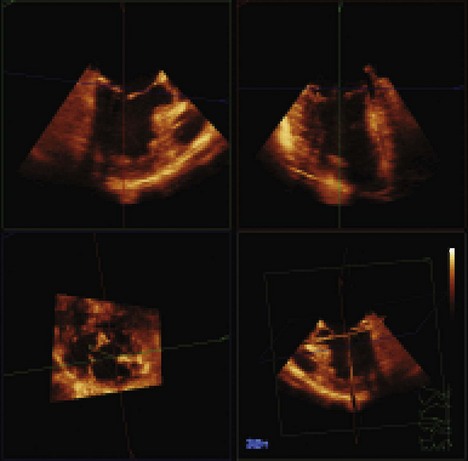
Three-dimensional (3D) TEE provides exceptional images of the heart. Instead of a plane of information, the computer acquires a volume of data, which can then be reconstructed and viewed from any angle (Figure 2-4). Moreover, the data set can be sliced in any desired plane, much like a computed tomography (CT) scan, in order to re-create 2D images sometimes impossible to obtain by standard 2D echocardiography (Figure 2-5).
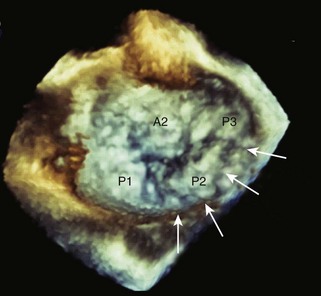
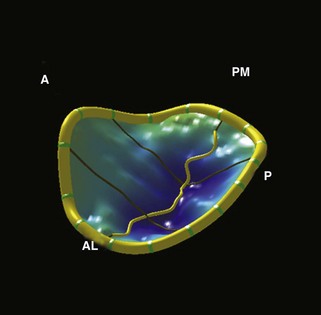
The mechanism of MR is usually readily apparent on 3D imaging. Furthermore, off-line MV analysis software packages allow detailed quantification of MV disease, including dimensions, prolapses, and restriction (Figure 2-6). This is very useful in planning the surgical management of MR and may help to identify patients who require specialized surgical care. Moreover, the development of leaflet stress analysis packages opens the door to the possibility of predicting, in the immediate post-bypass stage, the durability of some MV repairs.
Mitral Regurgitation
MR can be due to a structural problem in the valve itself or it may be due to distortion of the valve by external factors, described in Table 2-3.
TABLE 2-3 ETIOLOGY OF MITRAL REGURGITATION
| Structural MR | |
| Functional MR | |
| MR due to LVOT obstruction |
HOCM, hypertrophic obstructive cardiomyopathy; LV, left ventricle; LVOT, left ventricular outflow tract; MR, mitral regurgitation.
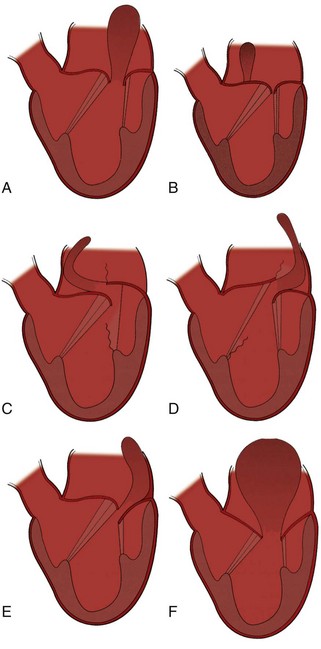
Classification of Mitral Regurgitation
Key Points
Evaluation of Mitral Regurgitation
Step 1: Determine the Mechanism and Localization of Lesions and Etiology
Key Points
Examination of the Mitral Annulus
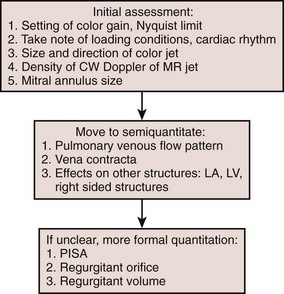
Flow chart of MR severity (Figure 2-8).
Severity of Mitral Regurgitation
Step 2: Qualitative Assessment
Color Flow Doppler