Chapter 31
Mitral Stenosis, Mitral Regurgitation, and Mitral Valve Prolapse
1. What is the usual cause of mitral stenosis (MS)?
2. What is the pathophysiology of MS?
MS inhibits the normal free flow of blood from left atrium (LA) to left ventricle (LV) in diastole. Normally, diastolic LA and LV pressures equalize shortly after mitral valve opening. In MS, the stenotic valve impedes LA emptying, inducing a diastolic gradient between LA and LV (Fig. 31-1). Elevated LA pressure is referred to the lungs, where it causes pulmonary congestion. Simultaneously, impaired LA emptying reduces LV filling, limiting cardiac output. Thus, the combination of increased LA pressure and decreased cardiac output produce the syndrome of heart failure. Because increased LA pressure increases pulmonary pressure, the right ventricle (RV) becomes pressure overloaded, eventually leading to RV failure.
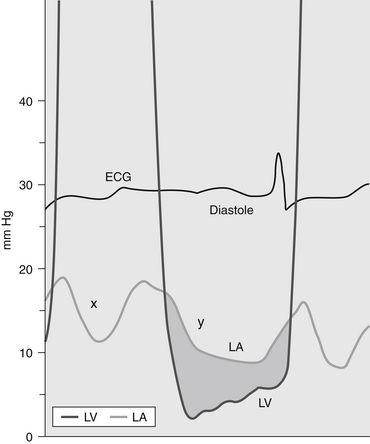
Figure 31-1 Pressure gradient in a patient with mitral stenosis. The pressure in the left atrium (LA) exceeds the pressure in the left ventricle (LV) during diastole, producing a diastolic pressure gradient (shaded area). (Modified from Bashore TM: Invasive cardiology: principles and techniques, Philadelphia, 1990, BC Decker, p. 264.) ECG, Electrocardiogram.
3. What are the typical symptoms of MS?
4. What are the signs of MS at physical examination?
5. How is the diagnosis of MS made?
Today, however, the echocardiogram is key to the diagnosis because it images the mitral valve so well. The valve is thickened and there is impaired opening of the mitral leaflets (Fig. 31-2). The LA is almost always enlarged. Valve area can be determined from direct visualization and planimetry of the mitral orifice, from Doppler assessment of the transvalvular gradient, and from measuring the delay in LA emptying. Pulmonary pressure, LV function, and RV function are also evaluated. In general, the main criteria for severe MS follow below. The severity of MS is estimated using the criteria given in Table 31-1.
TABLE 31-1
ECHOCARDIOGRAPHIC CRITERIA FOR THE ASSESSMENT OF THE SEVERITY OF MITRAL STENOSIS
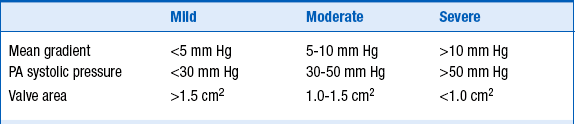
Modified from Bonow RO, Carabello BA, Chatterjee K, et al: ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. J Amer Coll Cardiol 48:e1-e148, 2006.
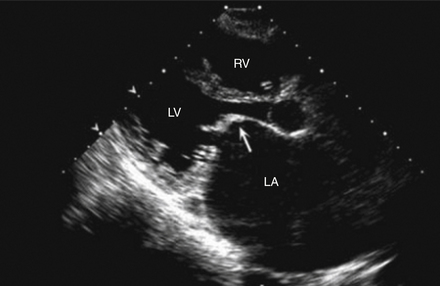
Figure 31-2 Two-dimensional echocardiogram of the parasternal long-axis view during diastole of a patient with mitral stenosis. The mitral valve leaflets are thickened and have the typical hockey-stick appearance (arrow). Note also that the left atrium (LA) is enlarged. LV, Left ventricle; RV, right ventricle. (Modified from Libby P, Bonow RO, Mann DL, Zipes DP: Braunwald’s heart disease: a textbook of cardiovascular medicine, ed 8, Philadelphia, 2008, Saunders.)



6. Is there effective medical management for MS?
7. What is the definitive management for severe MS?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


