Mitral annular calcium (MAC) is a common finding at echocardiography, although it is an unusual cause of severe mitral stenosis. Although MAC is known to be associated with atherosclerosis and chronic kidney disease, little is known about its natural history as affects mitral valve function. This report describes a cohort of 37 outpatients with severe MAC (>5 mm) of whom 32 were followed longitudinally with echocardiography (mean follow-up 2.6 ± 1.6 years). Progression of the mitral valve gradient occurred in 16 of 32 (50%). There was wide variation in rate of progression with a few subjects demonstrating a rapid increase in gradient, up to 9 mm Hg/year. Progression of mitral valve gradient correlated with baseline gradient at rest and with severity of overall cardiac calcification as measured by a semiquantitative echocardiographic score. Age at index echocardiogram was inversely related to mitral valve gradient after baseline, suggesting that calcification may proceed at a greater rate in younger patients. In conclusion, although severe mitral stenosis is uncommon in patients with MAC, those with a pre-existing gradient at rest and severe overall cardiac calcification appear to be at greater risk for development of this disease state.
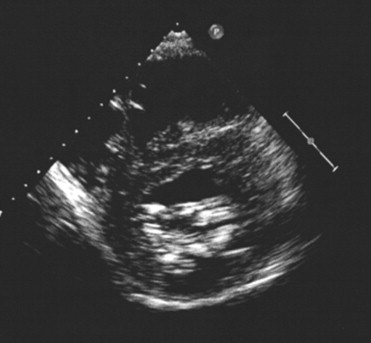
Mitral annular calcium (MAC) is an increasingly recognized cause of mitral valve gradients, particularly as the population ages. It can occasionally cause mitral stenosis (MS) severe enough to warrant valve replacement ( Figure 1 ). Compared to calcific aortic valve stenosis, little is known about the natural history of MS due to MAC. In this study a group of general cardiology outpatients with severe MAC was followed longitudinally with echocardiography to define the natural history of this disease.
Methods
Outpatient echocardiographic reports were searched for phrases regarding severe MAC; those with rheumatic disease or other identifiable mitral valve disease were excluded. All studies were performed in the setting of a private general cardiology practice from January 1, 2003 to October 1, 2005. This group has been previously reported. For this study, index echocardiograms were reviewed to confirm the presence of severe MAC, defined as MAC >5 mm in any dimension and occurring in the posterior annulus and/or anterior annulus (interannular fibrosa). Follow-up echocardiograms were obtained in all living patients who agreed to participate in the study. In addition, all identifiable interval echocardiograms performed for clinical reasons were obtained and reviewed. There were 37 participants with longitudinal follow-up in 32; 88 echocardiograms were reviewed of which 86 had acceptable Doppler recordings for measurement of mean mitral valve gradient. None had end-stage renal disease. This study was approved by the institutional review board at St. Francis Medical Center (Trenton, New Jersey).
For each echocardiogram, mean aortic and mitral valve gradients were recorded. A previously validated semiquantitative calcium score was applied and recorded ; this score looks at overall cardiac calcium on echocardiogram and specifically includes the aortic root and valve, the mitral annulus and interannular fibrosa, and the subvalvular apparatus. It has been shown to have a good correlation with cardiac calcification as judged by computed tomographic radiography.
For each subject, baseline glomerular filtration rate was calculated using the Modification of Diet in Renal Disease (MDRD) formula.
In statistical analysis, the variable representing mitral valve gradient was transformed using the natural logarithm. A multivariable random effects (mixed) model was used to determine the independent predictors of mitral valve gradient after baseline. All analyses were performed using STATA 10 (STATA Corp., College Station, Texas).
Results
Patients were followed for a mean of 2.6 ± 1.6 years. Results for the 32 subjects with longitudinal follow-up are presented in Table 1 . It should be noted that all echocardiograms were obtained at rest in stable patients. In no case was a change in mitral valve gradient due to high heart rate. In addition, no patient had significant (moderate or greater) mitral regurgitation. For the entire group mean mitral valve gradient progressed on average by 0.6 mm Hg/year (95% confidence interval −0.3 to +1.6). Progression was seen in 16 of 32 (50%). In those with progression, the average increase in mean mitral valve gradient was 2.0 mm Hg/year (median 0.6) but there was a wide range of progression (maximum observed increase 7 mm Hg over 271 days, approximately 9 mm Hg/year). Over the course of the study, 3 patients had or developed a mean mitral valve gradient at rest ≥10 mm Hg, consistent with severe MS (2 underwent mitral valve replacement), whereas 17 had or developed a mean gradient at rest ≥5 mm Hg, consistent with moderate MS. Echocardiographic calcium score increased on average 0.8 points/year (median increase 0.5).
| Age at Index Echocardiography/Gender | Months of Follow-up | Mean MV (mm Hg) | Echocardiographic Calcium Score (range 0–13) | Baseline AV Gradient (mm Hg) | GFR (ml/min/1.73 m 2 ) |
|---|---|---|---|---|---|
| 56/Female | 3 | 8 | 6 | AVR | 110 |
| 62/Female | 44 | 9 → 19 | 10 | 6 | 77 |
| 67/Male | 9 | 15 → 22 | 11 | 36 | 40 |
| 69/Female | 32 | 5 | 10 | 4 | 76 |
| 70/Female | 61 | 2 → 3 | 4 | 8 | 66 |
| 70/Male | 57 | 2 → 3 | 6 | 8 | 102 |
| 70/Female | 19 | 4 | 4 | 7 | 48 |
| 72/Female | 55 | 3 → 5 | 9 | 9 | 66 |
| 73/Male | 30 | 3 → 4 | 8 | 17 | 53 |
| 73/Male | 30 | 5 → 8 | 11 | 7 | 45 |
| 74/Male | 50 | 4 | 8 | 8 | 88 |
| 77/Male | 21 | 7 → 9 | 13 | 18 | 57 |
| 77/Male | 25 | 4 → 5 | 10 | AVR | 48 |
| 77/Male | 49 | 2 → 3 | 9 | AVR | 48 |
| 78/Female | 11 | 4 | 5 | 7 | 12 |
| 78/Female | 35 | 3 | 10 | 3 | 64 |
| 79/Male | 46 | 1 → 2 | 5 | 8 | 77 |
| 79/Female | 60 | 6 | 12 | 23 | 36 |
| 80/Male | 10 | 3 | 8 | AVR | 69 |
| 80/Female | 48 | 4 → 7 | 9 | 6 | 39 |
| 82/Female | 8 | 6 | 12 | 46 | 64 |
| 83/Male | 3 | 4 | 12 | 33 | 48 |
| 84/Female | 23 | 3 | 11 | AVR | 72 |
| 84/Male | 5 | 4 → 6 | 10 | 12 | 68 |
| 86/Male | 38 | 5 | 9 | 4 | 47 |
| 87/Male | 25 | 3 → 4 | 11 | 12 | 34 |
| 88/Female | 47 | 4 | 11 | 14 | 35 |
| 88/Male | 50 | 5 | 13 | 27 | 27 |
| 89/Female | 3 | 13 → 15 | 12 | AVR | 84 |
| 89/Male | 55 | 2 | 6 | 11 | 67 |
| 90/Female | 41 | 3 | 10 | 11 | 45 |
| 90/Male | 16 | 1 → 2 | 7 | 4 | 43 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


