Miscellaneous Phenomena Related to Atrioventricular Conduction
Concealed conduction, the gap phenomenon, and supernormality are physiologic events that may be considered to be variants of the normal response. These phenomena are responsible for many unusual or unexpected responses of atrioventricular (A-V) conduction. This chapter addresses these separate but interrelated phenomena of cardiac conduction.
Concealed Conduction
The definition of concealed conduction has been irrevocably altered by the availability of intracardiac electrophysiologic studies. The concept of concealed conduction, an explanation for the effects of incomplete penetration of an impulse into a portion of the A-V conduction system, was introduced (and then expanded on) by Langendorf1,2 and by Katz and Pick.3 The term was applied to unexpected phenomena observed on the surface ECG that were compatible with the effects of incompletely penetrating impulses that were not directly reflected on the surface ECG; hence the term concealed. Because intracardiac recordings can directly document the presence of these impulses during the electrophysiologic study, they are no longer truly concealed. Thus, specific consequences of incomplete penetration of impulses may be a less ambiguous term than concealed conduction of impulses to describe a variety of ECG findings.4 Although the A-V node is the structure with which concealed conduction has been most often associated, this phenomenon can occur in any portion of the A-V conduction system. The manifestations of concealed conduction (i.e., the effects of incomplete penetration of an impulse) include (a) unexpected prolongation of conduction, (b) unexpected failure of propagation of an impulse, (c) unexpected facilitation of conduction by “peeling back” refractoriness, directly altering refractoriness, and/or summation,4,5,6 and (d) unexpected pauses in the discharge of a spontaneous pacemaker. Excellent reviews of the ECG manifestations of concealed conduction are available.7,8,9,10,11
Concealed conduction may result from antegrade or retrograde penetration of an impulse into a given structure. The impulse producing concealment may originate anywhere in the heart – in the sinus node, an ectopic atrial site, the A-V junction, the fascicles, or the ventricles.7 The most common site manifesting the effects of concealed conduction is the A-V node. The effects of retrograde concealment in the A-V node under different circumstances are shown in Figures 6-1 through 6-4. Impulses from any subnodal site can produce concealed conduction. The ability of ventricular premature complexes (VPCs) to produce concealment in the A-V node depends on intact retrograde His–Purkinje conduction. In Figure 6-4, similarly coupled VPCs, manifesting different patterns of retrograde His–Purkinje conduction, have totally different effects on A-V nodal conduction of the sinus complex that follows. The effect of His bundle, fascicular, or ventricular extrasystoles on subsequent A-V nodal conduction is inversely related to the coupling interval of the premature depolarization. In patients with dual A-V nodal pathways (see Chapter 8), VPCs, fascicular premature complexes, and His bundle complexes can shift conduction from the fast to the slow pathway. Slow pathway can be maintained by retrograde invasion into the fast pathway (see Chapter 8). Retrograde concealment at multiple levels of the A-V conduction system may also occur (Fig. 6-5). The levels of concealment depend on the relative timing of antegrade and retrograde impulses.
The most frequent clinical circumstances in which concealed conduction is operative are: (a) atrial fibrillation during which the irregular ventricular response is due to the varying depth of penetration of the numerous wavefronts bombarding the A-V node8; (b) prolongation of the P-R(A-H) interval or production of A-V nodal block by a premature depolarization of any origin; (c) reset of a junctional (His bundle) pacemaker by atrial or subjunctional premature depolarizations; and (d) perpetuation of aberrant conduction during tachyarrhythmias. In the latter circumstance, retrograde penetration of the blocked bundle branch subsequent to transeptal conduction perpetuates aberration.12,13 This is the most common mechanism of perpetuation of aberration during supraventricular tachycardia observed in our laboratory (approximately 70% of cases). Wellens et al.14 have found a similar incidence of retrograde concealment producing perpetuation of aberration.
Concealed His bundle depolarizations can produce many unusual patterns of conduction, including simulation of type II second-degree A-V block (see Chapters 4 and 7). His bundle depolarizations are frequently not recognized because they must conduct antegrade and/or retrograde to have any
representation on the surface ECG. Incomplete penetration (concealment) of His bundle depolarizations in either direction, producing unexpected abnormalities of antegrade or retrograde conduction, may present a particularly difficult diagnostic problem.9,10 The intracardiac study may be extremely useful in assessing the causes and sites of concealed conduction by making all the components of the A-V conduction system available for analysis.
representation on the surface ECG. Incomplete penetration (concealment) of His bundle depolarizations in either direction, producing unexpected abnormalities of antegrade or retrograde conduction, may present a particularly difficult diagnostic problem.9,10 The intracardiac study may be extremely useful in assessing the causes and sites of concealed conduction by making all the components of the A-V conduction system available for analysis.
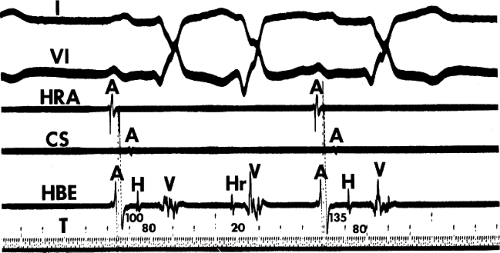 FIGURE 6-1 Retrograde concealed conduction by a fascicular extrasystole. From top to bottom, tracings represent standard leads 1 and V1 and high-right atrium (HRA), coronary sinus (CS), and His bundle electrogram (HBE) and time lines (T) at 10 msec and 100 msec. The first beat is a conducted sinus beat, with an A-H = 100 msec, H-V = 80 msec, and a right bundle branch block configuration. The second beat is a fascicular extrasystole, with an “Hr-V” = 20 msec. Note that there is no manifest conduction above the atrioventricular (A-V) junction (i.e., no atrial electrogram). Note, however, in the next sinus beat that the A-H interval is prolonged to 135 msec, indicating that the retrograde wavefront from the preceding beat partially penetrated (concealed) in the A-V node, rendering it relatively refractory to the next sinus impulse. A, atrial deflection; H, His bundle deflection; Hr, retrograde His deflection; V, ventricular deflection. |
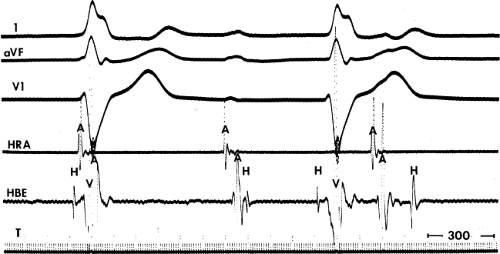 FIGURE 6-2 Retrograde concealed conduction by a junctional (His bundle) escape rhythm during intra-His complete heart block. A-V dissociation is present, and there is no retrograde activation of the atria by the His bundle escape rhythm. There are three sinus depolarizations, as evidenced by early high-right atrial (HRA) activation. The first sinus impulse is blocked above the proximal His bundle (i.e., in the atrioventricular [A-V] node), the second conducts to the proximal His bundle with a short A-H interval, and it is then blocked; and the third conducts to the proximal His bundle with a longer A-H interval. The A-V nodal block in the first beat and the A-V nodal delay in the third beat are due to concealed retrograde conduction of the His bundle beats into the A-V node. Thus, despite antegrade intra-His block, the distal His bundle escape rhythm can conduct retrogradely and affect antegrade conduction (i.e., unidirectional antegrade block is present). |
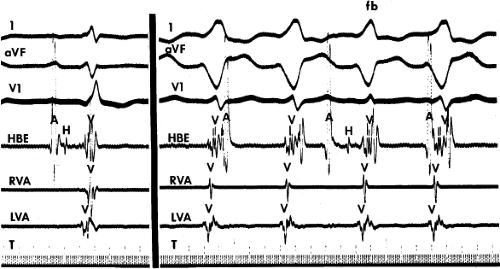 FIGURE 6-3 Retrograde concealed conduction during ventricular tachycardia. The tracing is arranged from top to bottom: surface ECG leads 1, aVF, and V1, His bundle electrogram (HBE), right ventricular apex (RVA), left ventricular apex (LVA), and time lines (T) at 10 msec and 100 msec. The left panel represents sinus rhythm. The right panel represents ventricular tachycardia without manifest retrograde conduction. Retrograde His bundle or atrial deflections are not seen. There are three sinus complexes, as reflected by atrial deflections (A) in the HBE tracing. Only the second results in a propagated response with a His bundle deflection (H) and a slight alteration in the QRS complex characteristic of a fusion beat (fb). Block of the first and third sinus impulses in the atrioventricular (A-V) node results from retrograde concealed conduction of the ventricular beats into the A-V node, rendering it refractory. |
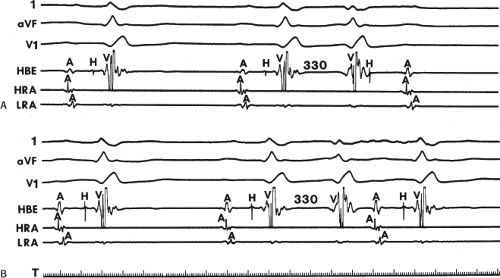 FIGURE 6-4 Concealed conduction by ventricular premature contractions (VPCs). A and B: Leads 1, aVF, and V1 and electrograms from the His bundle (HBE), high-right atrium (HRA), and low-right atrium (LRA). Sinus rhythm is present in the first two complexes of each panel. A: A VPC is observed at a coupling interval of 330 msec with retrograde conduction through the His bundle to the atrioventricular (A-V) node. This results in concealed conduction so that the subsequent sinus complex is a block in the A-V node. B: A similarly coupled VPD fails to reach the His bundle so that no concealment in the A-V node is manifested and the sinus complex conducts with a normal HV and normal A-H. Thus, the ability to produce concealed conduction in the A-V node by VPC depends on the ability to penetrate the A-V node via the His–Purkinje system. T, time line. |
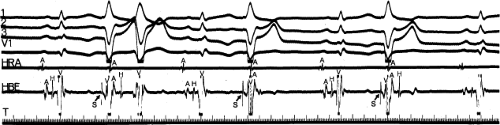 FIGURE 6-5 Multiple levels of concealed conduction during ventricular pacing. The rhythm is sinus, with ventricular pacing at a cycle length of 1200 msec (S, arrow). Following the first stimulated ventricular complex, the spontaneously occurring sinus impulse is conducted with a long H-V interval and left bundle branch block (LBBB) aberration. This indicates asynchronous concealment into both left and right bundle branches (long H-V and LBBB morphology). Following the second stimulated complex, the sinus impulse blocks in the A-V node, indicating concealed conduction to that structure. Following the third stimulated complex, the sinus impulse blocks below the His bundle, indicating concealment into the His–Purkinje system, rendering it totally refractory to the antegrade impulse. |
Although interference with normal antegrade conduction or with a subsidiary pacemaker by a concealed premature depolarization may be easy to conceptualize, unexplained facilitation of conduction requires further explanation. Most examples of facilitation of conduction (usually in the His–Purkinje system) can be explained by the premature impulse’s (a) allowing more time for the structure to recover excitability, which is due to peeling back the refractory period of that tissue, and/or (b) shortening the refractory period of tissues with cycle length-dependent refractoriness (i.e., the atria, His–Purkinje system, and ventricles) by decreasing the cycle length preceding the subsequent spontaneous impulse (Fig. 6-6) or retrograde conduction thru a site of antegrade block which both shortens the refractory period and allowing more time for recovery. Simultaneous shortening of refractoriness and providing more time to recover excitability is the most common mechanism. Abrupt normalization of aberration by a VPC (the finding of which proves retrograde concealment as the mechanism for perpetuation of aberration) is based on these principles (Figs. 6-7 and 6-8). Atrioventricular nodal conduction time and refractoriness may be shorted by VPCs delivered simultaneously with the prior atrial depolarization (Fig. 6-9). In an elegant study, Shenasa et al.15 demonstrated that VPCs shorten A-V nodal refractoriness and improve A-V nodal conduction at comparable coupling intervals at both long and short drive cycle lengths. One mechanism for this is summation, because VPCs without simultaneous atrial activation prolong refractoriness and slow conduction in the node. Another explanation would be for the VPC to produce earlier activation at the site of A-V nodal conduction delay or block. This allows more time for it to record when the APC is delivered. These and other mechanisms of facilitation explain some instances of pseudo-supernormal conduction.
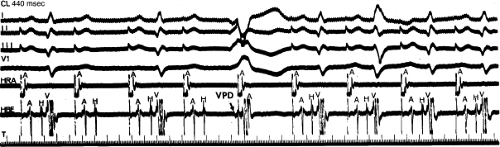 FIGURE 6-6 Facilitation of His–Purkinje conduction by a ventricular premature depolarization (VPD). During atrial pacing at a cycle length of 440 msec, 2:1 block below the His bundle occurs. A VPD (arrow) is introduced just before the fifth atrial paced complex. Following the VPD, the P wave that should block in the 2:1 sequence conducts with the same A-H and H-V intervals as other conducted complexes. Facilitation of His–Purkinje conduction results because the VPD “peeled back” His–Purkinje refractoriness, allowing the atrial impulse to propagate through the previous site of block. See text for discussion. (From Gallagher JJ, Damato AN, Varghese PJ, et al. Alternative mechanisms of apparent supernormal atrioventricular conduction. Am J Cardiol 1973;31:362.)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|