14
Metal industry and related jobs (including welding)
Work in metal industries results in exposures both to metals and to nonmetal materials. Respiratory effects of oil-containing solutions known as metal working fluids, which are widely used in shaping and cutting metals with tools, are discussed in detail in chapter 16 by Rosenman, on the automobile industry.
Metals are elements. There are approximately 91 distinct metals in the periodic table. Each one may have a number of different valences and oxidation states. The different forms (i.e. oxidation states) may markedly affect metals’ effects on the lungs and other organs. Exposure in the workplace is usually to aerosols (small metal particles), and in some cases vapor, such as mercury, which is readily evaporated at room temperature. As elements, metals cannot be broken down or converted to other substances under usual conditions, so they are environmentally persistent. In usual practice, metals cannot be destroyed, but only moved from one place to another or combined into compounds. Mixtures made from two or more metals are alloys. Even after being burned, buried or recycled, metals can continue to affect the health of workers and the public. Metals can also be easily measured in workplace air by industrial hygienists, both by total weight and by particle size-specific fractions.
Measurement of the concentration of certain metals in urine or blood may be a useful indicator of recent exposures, either environmental or occupational, and testing is readily available from certified laboratories. Some metals which are less soluble in biological fluids are persistent in the lungs and other organs, and may be measured in biopsy or autopsy specimens.
14.3 Workplace hazards from metals
While all substances are toxic to the lungs in sufficiently high doses, the large amounts of metals used widely in industry, and their dose-response toxicity, have identified beryllium and cobalt as frequent causes of serious occupational lung disease. Most metals are solid at room temperature and are converted to gas only at very high temperatures. When metal gas condenses in air, small particles of the metals combined with oxygen (metal oxide fume) result. Freshly formed fume particles are small enough to be inhaled and deposited in small airways and alveoli. Such small particles agglomerate rapidly in air to form larger particles. If the patient worked close to the source of fume formation, clinically significant amounts of metal may have been inhaled as fume particles. For this reason, an occupational exposure history of prolonged work with metals exposed to very high temperatures, or to very high mechanical forces, is suggestive of a workplace where larger amounts of metal inhalation may have occurred.
Respiratory exposure to metals may occur in each of the common processes of the metal industry. Mining is the process of removing metals from their natural site of origin in the earth. The more significant risk of lung disease for metal miners may be from silica. Silica is the most common compound in the earth’s surface, and miners must often dig through silica-containing rock to extract the metal ore they seek. Inhaled crystalline silica may cause chronic mucous expectoration (chronic bronchitis), chronic airflow obstruction, nodular interstitial lung disease with pleural thickening, silicaproteinosis (a form of pulmonary alveolar proteinosis) and enlarged pulmonary and systemic lymph nodes. Silicosis predisposes to the development of active tuberculosis and also to lung cancer. Silica may also be a mixed exposure, with the metal ore being mined. Mixed dust pneumoconiosis closely resembles silicosis, but is distinguished by the predominance of nonsilica dust fibrotic lesions over silicotic nodules. This may occur in metal miners and others with mixed mineral dust exposure. Miners may also develop systemic medical toxicity from mercury, lead and manganese when exposures are of sufficient intensity and duration.
Metal ores removed from the earth are often mixtures of the metal with other minerals which must be separated. Exposure to the metal itself, or to other metals present in the ore mined, may occur during these processes.
Milling refers to the processing of metal ores (mixtures of metals with other minerals) to separate the component desired, and often involves mechanical crushing and heating the ore. Metal ore is separated from other mined minerals in a mill. Smelting is the process by which a metal is separated from its ore by using a chemical reducing agent to change the oxidation state of the metal. In a foundry metal is heated to a liquid form, and poured into a mold to form it into useful shapes. Silica sand is often used for this process and may be a hazardous source of silica dust exposure. Silica sand or other granular molding materials may contain a binder made with isocyanates or furans, which can cause respiratory sensitization and asthma. Forging deforms metal to a given size and shape using hot or cold processes. Grinding, polishing and buffing remove excess metal, or smooth and shape the metal surfaces, and may lead to inhalation exposures of materials used to accomplish these (such as grinding wheels) as well as the metal being shaped. Metal machining processes further shape the metal parts using a variety of cutting, drilling and surfacing tools, often with the use of metalworking fluids to cool and lubricate the process. These processes may produce an aerosol of metal particles and the aerosolized metalworking fluids may serve as a vehicle for metal particles or metal in solution, as well as their own inhalation effects. Electroplating produces a thin layer of metal on another surface by a process of electrical-chemical bonding of metal in a tank with metal salt solutions. Galvanization coats a thin layer of zinc oxide on steel either by an electroplating process or by dipping steel in molten zinc. Metals may also be applied to surfaces by the processes of combustion, detonation, plasma, and electric arc spraying, with resulting exposure to metal fume. Exposure to metals may also occur when products are scrapped, incinerated, reclaimed or recycled. Those performing these processes may have no way of knowing which metals they are exposed to. Inhalation exposure may occur in many intermediary processes using metals, and skin exposure may be important to the development of beryllium lung disease.
14.4.2 Steel structures, ship building, and shipbreaking
Many large buildings and all ships are steel structures built to withstand extreme mechanical stress and a relentlessly oxidizing environment. Steel structures also include bridges, land-based liquid holding tanks, submarines, oil drilling platforms, airplanes and trains. Making such structures results in steel and other metal exposures both in producing the parts and in assembling them. Such structures are commonly built using welding and a variety of other assembly techniques. When these structures finish their useful life, they are torn down and the metal often cut apart for metal recycling using high-temperature torches. Exposures again occur in these processes, often in circumstances where the other constituents of the structures are unknown.
14.5 Pulmonary responses to metals
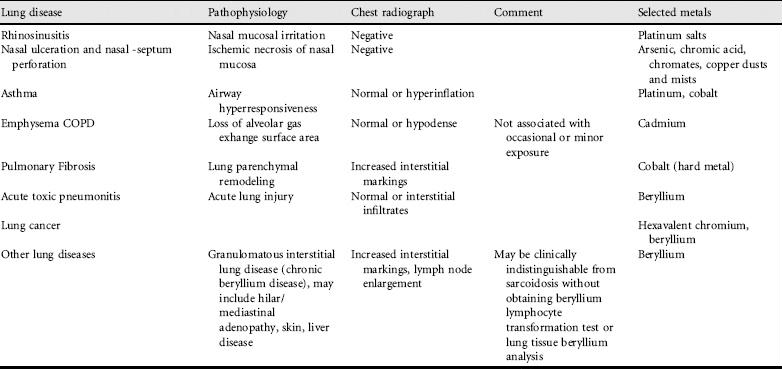
Metals cause a broad spectrum of common respiratory conditions – rhinosinusitis, nasal septal perforation, laryngeal disease, acute and chronic bronchitis, asthma, emphysema, pulmonary fibrosis, granulomatous lung disease (chronic beryllium disease) and lung cancer (Table 14.1). Most cases of metal-induced lung diseases are nonspecific (i.e. no pathological characteristics identifying them as occupationally induced). Metal dust might be one of the environmental factors predisposing to the development of fibrosing alveolitis (usual interstitial pneumonia, idiopathic pulmonary fibrosis). There are also some metal-induced lung diseases which have distinctive characteristics (see chronic beryllium disease and giant cell interstitial pneumonia, below).
Most metal particles can cause chronic bronchitis if particles small enough to penetrate to the large bronchi are inhaled with sufficiently intense and prolonged exposure. Clinically important toxicity to other organ systems may occur from metals which pass into the blood after being inhaled into the lungs. Lead affects peripheral nerves, brain and bone marrow; mercury affects peripheral nerves, brain and kidneys; cadmium is toxic particularly to kidneys; arsenic to the gastrointestinal system, peripheral nerves and skin; and manganese affects brain.
Many metals, when inhaled in particle sizes small enough to be deposited and retained in the lungs, can cause dust macules, which are collections of dust and dustladen macrophages around small airways and vessels. If unaccompanied by a reaction of the lungs, these macules may be entirely asymptomatic, although they may create a pattern of densities on chest radiographs or other lung images. The prominence of lesions seen on chest radiograph is related in part to the radiodensity of the dust, so that some macules with no associated lung fibrosis but high intrinsic radiodensity can produce a strikingly abnormal radiograph with little or no functional loss. Inhaled barium dust is one such metal which produces this result. Other metals and dusts may cause significant loss of lung function with much less prominent chest radiograph abnormalities. Silica is associated with increased risk for collagen vascular disease. Use of complete pulmonary function testing, including spirometry, lung volumes and diffusing capacity, is the most accurate means of assessing residual lung function.
Two specific metals and an important metal processes deserve special mention as causes of serious and sometimes characteristic lung disease.
14.6 Beryllium: lung and systemic effects
The metal beryllium is much lighter than aluminum, stiffer than steel, has a high melting point and will hold its shape over a wide temperature range. It may be used where there is need for a combination of good electrical conductivity, high strength, wear resistance, high fatigue strength and nonmagnetic and nonsparking properties.
It has an unusual property of reflecting neutrons emitted from plutonium, which makes beryllium an essential component of nuclear weapons and nuclear reactors. Beryllium oxide is used to make light, strong industrial ceramic insulators. Beryllium is often alloyed with copper, aluminum and other metals. The metal has many applications in industrial and consumer product manufacturing. Selected common applications are electronic connectors, contact springs, switches, relays, metal diaphragms, friction wear parts, bushings and bearings, actuators, welding electrodes and plastic injection mold components.
Major beryllium metal production facilities have existed in recent years in the USA, Khazakstan and China. Major manufacturing facilities for beryllium and berylliumalloys are located in the USA, Japan and France, and chronic beryllium disease has been well described in manufacturing workers. The beryllium metal, oxide and alloys produced are utilized worldwide in a large variety of applications including military and consumer electronics, cell phones and microprocessors to name only a few. Clinically significant exposure to beryllium may occur when processing beryllium alloy into consumer products (such as when drilling, grinding, or machining the alloy) or when recycling or reclaiming metals containing beryllium using a furnace to melt them. Exposure may also occur when welding beryllium metal using beryllium-containing welding rods.
When inhaled into the lungs beryllium can cause a chronic, T-cell mediated granulomatous disease involving lung, lymph nodes and sometimes skin, liver and other organs, that may have its clinical onset many years after first occupational exposure to beryllium dust. This usually slowly progressing condition is known as chronic beryllium disease (also known as berylliosis).
A minority of workers exposed to beryllium develop chronic beryllium disease, and there is an important interaction between certain gene polymorphisms and exposure to the metal with regard to risk for disease. Because beryllium is expensive in comparison with other metals, recognized cases of beryllium disease have clustered around identified industrial facilities making beryllium metal or products from beryllium metal, nuclear weapons manufacturing facilities and operations recycling metal-containing electronic equipment. Because of the difficulty in diagnosis, it is difficult to estimate how many cases of beryllium disease occur annually. Investigators in Germany and Israel concluded that 13% of their patients with a previous diagnosis of sarcoidosis who were tested had chronic beryllium disease based on positive lymphocyte transformation tests for beryllium. However, worldwide use of beryllium has increased over time, suggesting that disease will continue to occur.
Testing of exposed industrial groups with the beryllium lymphocyte transformation test can identify individuals with T-lymphocytes sensitized to beryllium even when they have no manifestations of disease. Clinical follow-up of these individuals over several years shows that some will go on to develop chronic beryllium disease, although it is not yet known whether all such individuals, or what proportion of those with sensitization, would develop disease with sufficient follow-up. Thus, asymptomatic individuals with positive beryllium lymphocyte transformation tests are at risk for developing chronic beryllium disease. For patients with progressive clinical disease, some experts recommend lifelong systemic corticosteroid therapy (e.g. prednisone, 0.5-0.6 mg/kg per day in divided doses) to prevent or slow progression of disease. Methotrexate has been used as a steroid-sparing agent. Controlled trials are not available to address the question of whether corticosteroid or methotrexate treatment improves prognosis or survival.
Patients with chronic beryllium disease often present as adults with hilar or mediastinal adenopathy and patchy interstitial lung disease which is clinically recognized years after first exposure – a picture that usually cannot be distinguished from sarcoidosis based on standard clinical approaches. Lung biopsy shows noncaseating granulomas comparable to those of sarcoidosis. Patients with chronic beryllium disease often receive the diagnosis of sarcoidosis before the correct diganosis is made. Chronic beryllium disease can be distinguished by a history of beryllium exposure with an appropriate time interval of latency, and positive beryllium lymphocyte transformation tests of peripheral blood or bronchoalveolar lavage fluid. Clinical lymphocyte transformation testing is available from several reference laboratories in Europe and North America. Quantitation of the weight of beryllium metal per gram of ashed lung tissue from a large biopsy or autopsy specimen was used to confirm diagnosis before the availability of lymphocyte transformation testing.
Inhalation of beryllium fume from heating the metal to high temperatures can cause severe or fatal acute toxic pneumonitis.
14.7 Cobalt disease (hard metal pulmonary disease)
Cobalt causes lung disease alone and when combined with tungsten in a preparation known as ‘hard metal’, composed of sintered tungsten carbide with cobalt. (Sintering is a process of combining metal powders under pressure into a hardened product.) Cobalt may cause occupational asthma or an acute or chronic interstitial lung disease which may have a distinct pathology originally described as giant cell interstitial pneumonitis. The onset of interstitial fibrotic lung disease may be while working with the metal, or with a period of latency after exposure. Pulmonary function testing may show a restrictive, obstructive or mixed pattern usually with reduced diffusing capacity. The course of the interstitial lung disease is variable, sometimes with early or late remission, although sometimes with progression to respiratory failure and death. As with beryllium disease, cases of hard metal or cobalt lung disease are sporadic among those exposed at work, but no gene polymorphisms associated with increased or decreased susceptibility have been identified.
14.8 Welding-related lung disease
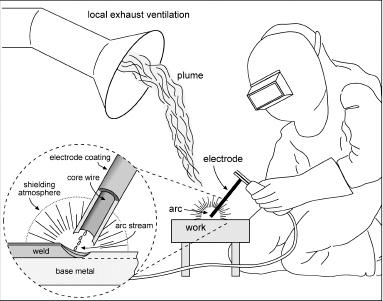
Welding is defined as any process of joining pieces of metal that have been made soft or liquid by heat or pressure. The occupation of welder is a skilled and relatively highpaying one that is growing rapidly worldwide to meet the need for more large, strong, fabricated structures. Although welding techniques are numerous, many of them produce significant lung exposures, including the most common one, manual metal arc welding. Typically in this process the welder must closely watch the weld from a distance of only 50 cm (Figure 14.1), and thus can easily inhale the welding plume given off by the process. The eye protection necessary to prevent damage from light and particles is not sufficient to protect from inhalation exposures, and welders often do not wear separate respiratory protection. Inhalation of the gas and particle components of the welding plume is thus likely unless measures are taken to capture or divert the plume away from the welder’s breathing air. Spot welding is a mechanized process in which the period of welding is brief, and the operator of the welding machine may be at a greater distance from the source of the plume.
Figure 14.1 Process of manual metal arc welding. Manual metal arc welding, the most widely used welding technology, uses an electric arc across an air gap between base metal (the material being joined together, here labeled ‘work’) and filler metal (the material used to make the electrode). The welder must usually visualize the process, through ultraviolet-filtering lenses to protect the eyes, from arm’s-length to assure the quality of the weld. The process creates the welding plume consisting of vaporized metal which rapidly forms fine metal-oxide fume particles, and gases. The largest metal component of the plume comes from the filler metal making up the welding ‘stick’ or filler ribbon, here labeled ‘electrode’. The components of the plume are usually multiple and complex. Heat from welding can convert nitrogen-containing materials coating the metal, or nitrogen in air, to nitrogen oxides, and ultraviolet light from the arc can convert oxygen to ozone. Exposures to these gases in enclosed spaces can be sufficient to cause acute lung injury. Local exhaust ventilation is usually needed to control exposures indoors. [Inset] To make a stronger weld without oxidation of the metal, welding processes exclude oxygen from the point of joining metal. Manual metal arc welding electrodes are coated with materials which create a gaseous shielding atmosphere as the electrode is consumed, keeping oxygen out. Droplets of molten metal from the electrode follow the path of electrons from electrode to the work (the arc stream) filling the weld with metal derived from the electrode fume. Depending on the welding process and the ventilation conditions, the airborne exposures during welding can be very high, or very low. In an enclosed space, standards for particle exposures may be exceeded within a few minutes. Welders may also be exposed to metal particles when they grind the weld to smooth the surface, when they burn through paints and coatings containing metals (such as lead), or from bystander exposures to other processes. In the most common welding processes, metal exposure may come from the base metal, the metal coating on the work piece, the electrode and fluxes, but the majority of the metal inhalation exposure comes from the welding electrode or wire. It is thus important to know the constituents of the electrode (which are often complex) as well as of the base metal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


