The incidence and clinical correlates of acute in-hospital mortality of takotsubo cardiomyopathy (TTC) are not clear. We performed a systematic review and meta-analysis to consolidate the current evidence on acute mortality in TTC. We then assessed the impact of “secondary” TTC, male gender, advancing age, and catecholamine use on mortality. A comprehensive search of 4 major databases (EMBASE, Ovid MEDLINE, PubMed, and Google Scholar) was performed from their inception to the first week of July 2013. We included original research studies, recruiting ≥10 participants, published in English language, and those that reported data on mortality and cause of death in patients with TTC. Of 382 citations, 37 studies (2,120 patients with TTC) from 11 different countries were included in the analyses. The mean age of the cohort was 68 years (95% confidence interval [CI] 67 to 69) with female predominance (87%). The in-hospital mortality rate among patients with TTC was 4.5% (95% CI 3.1 to 6.2, I 2 = 60.8%). Among all deaths, 38% were directly related to TTC complications and rest to underlying noncardiac conditions. Male gender was associated with higher TTC mortality rate (odds ratio 2.6, 95% CI 1.5 to 4.6, p = 0.0008, I 2 = 0%) so was “secondary” TTC (risk difference −0.11, 95% CI −0.18 to −0.04, p = 0.003, I 2 = 84%). The mean age of patients dying tended to be greater than that in the whole cohort (72 ± 7 vs 65 ± 7 years). In conclusion, TTC is not as benign as once thought. To reduce the mortality rate, greater efforts need to be directed to the diagnosis, treatment, and ultimately prevention of “secondary” TTC.
Takotsubo cardiomyopathy (TTC) is an acute cardiac condition that affects aging women and has a generally favorable prognosis. However, cardiac complications are common in the acute stage of the disease. Only 1 recent major study has evaluated the in-hospital mortality related to TTC in the American population by diagnosing TTC from National Inpatient Sample discharge database using International Classification of Diseases. However, this method is prone to coding errors and wrong diagnosis. In addition to that, information on mortality comes from small case reports. We therefore performed a meta-analysis and systematic review to determine the global incidence of in-hospital mortality and consolidate the evidence. In the present study, we sought to determine using a systematic review and meta-analysis approach: (1) the “overall” risk of in-hospital mortality in patients with TTC and (2) clinical correlates of variability in this risk. In addition, we prospectively elected to evaluate in particular the putative impact of (1) TTC occurring secondary to other life-threatening disorders, (2) TTC in men, (3) advanced age, and (4) TTC precipitated by medication-induced increases in catecholamine levels.
Methods
This systematic review and meta-analysis is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement guidelines. We included comparative studies of any design (randomized control trials, cohort, case control, and cross sectional). Eligible studies had to provide documentation on the in-hospital mortality rate in patients diagnosed with TTC and the mode of death for all the patients who died in hospital after a diagnosis of TTC. Furthermore, only studies with ≥10 patients were considered eligible. Inclusion was restricted to publications in the English language or when translation of the foreign language publications was provided. When data were reported from overlapping study samples (e.g., multiple publications from the same group), the most recent study or the one with the highest number of patients was included in the analysis. Single case reports and previous systematic reviews on TTC were not included.
For the purpose of this meta-analysis, we defined “secondary TTC” as development of TTC in a patient already suffering from a potentially life-threatening medical and/or surgical condition and “primary TTC” as that which developed in the absence of such acute critical illness.
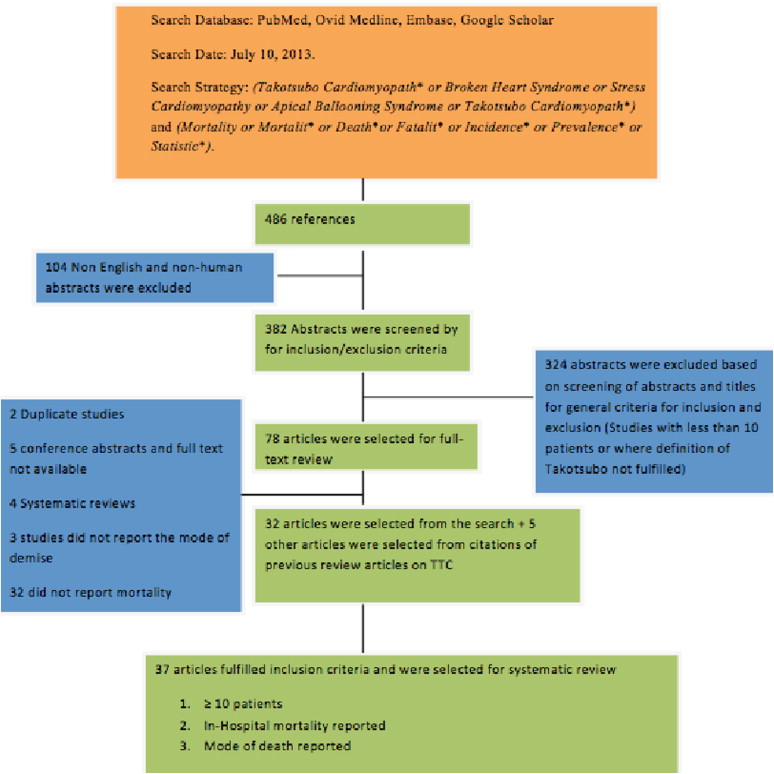
A comprehensive search strategy was designed with the assistance of an expert librarian from the University of Adelaide. A thorough computer-based search was performed using Ovid MEDLINE, EMBASE, Google Scholar, and PubMed databases. Search terms included (Takotsubo Cardiomyopath* or Broken Heart Syndrome or Stress Cardiomyopathy or Apical Ballooning Syndrome or Takotsubo Cardiomyopathy) and (Mortality or Mortalit* or Death*or Fatalit* or Incidence* or Prevalence* or Statistic*). No limit to the start date was applied, and the search was conducted up to July 10, 2013. We hand searched the references cited in the previous reviews and important articles on TTC. We contacted the corresponding authors of the studies in which relevant information was missing.
Two reviewers (KS and KC) screened all titles and abstracts independently. This was followed by the full-text review of the selected articles by the same 2 reviewers. One reviewer (KS) extracted data independently from selected studies using a standardized, pilot-tested, extraction template. The following data were extracted: study characteristics (author, country, study design, study population, number of participants, and objective of the study), participant characteristics (age and gender), clinical characteristics (acute coronary syndrome type for TTC, predisposing physical and/or emotion stressors, left ventricle ejection fraction, and acute complications), in-hospital mortality (number of in-hospital deaths and mode of demise), and predictors of mortality and acute complications.
Two independent reviewers (KS and RS) assessed the quality of included studies using a subset of the report by Tooth et al titled “Quality of Reporting of Observational Longitudinal Research,” including only the 23 quality domains relevant to a meta-analysis of observational studies. We assessed biases using classifications of “low risk of bias” when data for the criterion were reported, “high risk of bias” when data were not reported, and “unclear risk of bias” when the criterion was not relevant to the study design. Review Manager (RevMan, Computer program, Version 5.2., Copenhagen, The Nordic Cochrane Centre, The Cochrane Collaboration, 2012), was used to generate the risk of bias graph. Disagreements between reviewers for classifications were resolved by either consensus or inclusion of a third party (KC).
Continuous variables are reported as mean ± SD, whereas skewed data are described as median ± interquartile range. Categorical variables are reported using odds ratios (ORs) with 95% confidence intervals (CIs). Risk estimates are presented using OR, risk ratio, and risk difference with 95% CI. Heterogeneity between studies was assessed by a combination of the I 2 statistic, Cochran’s Q test, and observation of the data for each outcome. If formal meta-analysis was not possible because of a skewed distribution of the number of patients between each study, we disregarded the individual studies and used data as if obtained from a single study. Studies with missing data were excluded from meta-analyses and details extrapolated in the quality and risk of bias assessments. We then used logistic regression to assess the relation. Significant interaction between variables was considered when p <0.05. All calculations were performed using Review Manager software, version 5.2.
Results
The literature search on TTC and mortality yielded 486 citations ( Figure 1 ), of which 382 citations were in English and were related to humans. Abstracts were reviewed for the 382 short listed citations, and 78 reports were chosen for full-text review. Of the 78 full-text manuscripts reviewed for eligibility, 32 met all the inclusion and exclusion criteria. An additional 5 manuscripts were identified through hand searching, leading to a total of 37 studies included in this analysis. Five authors were contacted for missing data, with one responding and providing the requested information.
All the study designs were observational, including 22 retrospective studies, 13 prospective, and 2 partially retrospective and partially prospective studies. Sample size ranged from 10 to 256 participants (total 2,120). Fifteen of these studies were from Europe, 13 were from Asia, 8 were from the United States, and 1 from Australia.
Basic characteristics of the patients are detailed in Table 1 . Among the whole cohort of 2,120 patients with TTC, 87% (n = 1,859) were women. The mean age of patients diagnosed with TTC was 68 years (95% CI 67 to 69). There was a significant association between the presence of physical and/or emotional stress and development of TTC (OR 6.23, 95% CI 4.04 to 9.63, p <0.00001, 27 studies, I 2 = 85%; Supplementary Figure 1 ). Approximately 52% of patients presented as non–ST elevation myocardial infarction rather than ST elevation myocardial infarction. Chest pain (63.4%) was the most common presenting symptom followed by dyspnea (23.2%). In 13.3% of patients, the mode of presentation was incidental finding of abnormal electrocardiogram, syncope, palpitations, hypotension, shock, and vomiting.
| No. | First Author | Year of Publication | Country | Patients With TTC | Age (yrs) | Gender | ACS Type | Variant of TTC | Left Ventricular Ejection Fraction (%) | Emotional/Physical Stress | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | STEMI | NSTEMI | Typical | Atypical | Index Event | Follow-Up | Present | Absent | ||||||
| 1 | Spedicato | 2008 | Italy | 29 | 64 ± 12 | 4 | 25 | 18 | 11 | 29 | 0 | 32 | 60 | 9 | 20 |
| 2 | Elian | 2006 | Israel | 13 | 68 | 1 | 12 | 12 | 1 | 13 | 0 | 38 ± 5 | 65 ± 5 | NA | NA |
| 3 | Bonello | 2007 | France | 14 | 68 ± 15 | 1 | 13 | 6 | 8 | NA | NA | 40.6 ± 7.2 | 56 ± 5.2 | 6 | 8 |
| 4 | Buja | 2012 | Italy | 54 | 72.1 | 7 | 47 | 41 | 13 | 40 | 14 | 41 ± 10 | 67 ± 6 | 20 | 34 |
| 5 | Hsu | 2010 | Taiwan | 12 | 72 ± 10 | 0 | 12 | 9 | 3 | 9 | 3 | 59 ± 11.5 | 5 | 7 | |
| 6 | Sato | 2006 | Japan | 16 | 71.5 ± 9.4 | 1 | 15 | 9 | 7 | NA | NA | 40 ± 8 | 62 ± 5 | NA | NA |
| 7 | Azzarelli | 2009 | Italy | 19 | 65 ± 13 | 2 | 17 | 9 | 10 | NA | NA | 40 ± 7 | 60 ± 4 | 5 | 14 |
| 8 | Valbusa | 2008 | Italy | 22 | 76 ± 7 | 0 | 22 | 9 | 13 | 22 | 0 | 40.9 ± 12.4 | NA | NA | NA |
| 9 | Kwon | 2012 | South Korea | 208 | 65.8 ± 14.0 | 57 | 151 | 54 | 154 | 140 | 68 | 45.6 ± 15.5 | NA | 33 | 175 |
| 10 | Primetshofer | 2010 | Australia | 31 | 75 ± 10.2 | 3 | 28 | 13 | 18 | NA | NA | 41 ± 7 | 62 ± 5 | 7 | 24 |
| 11 | Eshtehardi | 2009 | Switzerland | 41 | 65 ± 11 | 6 | 35 | 16 | 25 | 33 | 8 | NA | NA | 16 | 25 |
| 12 | Jabara | 2009 | United States | 38 | 64 ± 12 | 6 | 32 | 19 | 19 | 29 | 9 | NA | NA | NA | NA |
| 13 | Song | 2010 | South Korea | 87 | NA | 23 | 64 | 28 | 59 | NA | NA | 40 ± 13 | 61 ± 7 | 20 | 67 |
| 14 | Elesber | 2007 | United States | 100 | 66 ± 13 | 5 | 95 | 33 | 67 | NA | NA | 33 (26–39) | 59 (55–63) | 44 | 56 |
| 15 | Lee | 2010 | South Korea | 56 | 64 (52–74) | 15 | 44 | 16 | 40 | 48 | 8 | 43 ± 12 | 61.26 ± 8.77 | 17 | 39 |
| 16 | Vriz | 2013 | Italy | 25 | 66.8 ± 11.76 | 4 | 21 | 20 | 5 | 10 | 15 | 32 ± 11 | NA | 9 | 16 |
| 17 | Sharkey | 2010 | United States | 136 | 68 ± 13 | 6 | 130 | 67 | 69 | NA | NA | 36 ± 9 | >50 | 15 | 121 |
| 18 | Parodi | 2011 | Italy | 116 | 73 ± 10 | 10 | 106 | 70 | 46 | NA | NA | NA | NA | 37 | 79 |
| 19 | Kurisu | 2010 | Japan | 102 | 74 | 13 | 89 | 80 | 22 | NA | NA | 42.5 ± 9.3 | NA | NA | NA |
| 20 | Joe | 2012 | South Korea | 37 | 66.1 ± 15.6 | 10 | 27 | 6 | 31 | 31 | 6 | 33 ± 13 | 59 ± 5 | NA | NA |
| 21 | Ionescu | 2010 | United States | 27 | 68 ± 14 | 1 | 26 | 15 | 12 | 20 | 7 | 50.4 ± 12.9 | 68 ± 12 | 6 | 21 |
| 22 | Kurowski | 2007 | Germany | 35 | 71.6 ± 8.7 | 2 | 34 | 24 | 11 | 22 | 13 | 41 ± 9 | 59 (7) | 5 | 30 |
| 23 | Previtali | 2011 | Italy | 128 | 67 ± 11 | 3 | 125 | 49 | 79 | 105 | 23 | 47 | 66.3 ± 6 | 53 | 75 |
| 24 | Eitel | 2011 | Europe/North America | 256 | 69 ± 12 | 29 | 227 | 108 | 148 | 197 | 42 | 42.2 ± 7.3 | 64.4 ± 7.3 | 74 | 182 |
| 25 | Akashi | 2004 | Japan | 10 | 72.9 | 1 | 9 | 9 | 1 | NA | NA | 44 ± 12 | 53 ± 11 | NA | NA |
| 26 | Burgdorf | 2008 | Germany | 50 | 70 ± 10 | 3 | 47 | 27 | 23 | 32 | 18 | 28 ± 10 | 51 ± 14 | NA | NA |
| 27 | Vidi | 2009 | United States | 34 | 66 ± 14 | 2 | 32 | 22 | 12 | 14 | 20 | 41 ± 11 | 64 ± 10 | 9 | 25 |
| 28 | Tsuchihashi | 2001 | Japan | 88 | 67 ± 13 | 12 | 76 | 79 | 9 | NA | NA | 37 ± 12 | 59 ± 7 | 26 | 62 |
| 29 | Regnante | 2009 | United States | 70 | 67 ± 11 | 3 | 67 | 29 | 41 | 68 | 2 | 41 ± 11 | 58 ± 8 | 23 | 47 |
| 30 | Singh | 2010 | United States | 114 | 66 ± 14 | 8 | 106 | 22 | 92 | 58 | 49 | 32 | 65 | NA | NA |
| 31 | Yoshioka | 2008 | Japan | 34 | 64 ± 17 | 12 | 22 | 25 | 9 | 26 | 8 | NA | NA | NA | NA |
| 32 | Mitsuma | 2010 | Japan | 21 | 72 | 3 | 18 | 15 | 6 | NA | NA | 42.50 | 70 | 4 | 17 |
| 33 | Herting | 2006 | Germany | 32 | 67.5 | 3 | 29 | 12 | 20 | NA | NA | 40 | 60 | 19 | 13 |
| 34 | Lee | 2009 | Singapore | 10 | 55 | 4 | 6 | 6 | 4 | NA | NA | 42.60 ± 6.67 | 53.88 ± 6.71 | 0 | 10 |
| 35 | Fang | 2008 | Taiwan | 10 | 65 ± 17 | 4 | 6 | 5 | 5 | NA | NA | 59 | 4 | 6 | |
| 36 | Mitchell | 2007 | United States | 22 | 0 | 22 | 13 | 9 | 22 | 0 | NA | NA | 4 | 18 | |
| 37 | Athanasiadis | 2006 | Germany | 23 | 65 ± 10 | 1 | 22 | 16 | 7 | NA | NA | NA | NA | 4 | 19 |
According to the wall motion abnormalities, although TTC occurs relatively frequently as apical and midventricular forms, 20 studies specified the regional pattern of TTC of these; apical TTC was found in 75% (n = 939) and other variants were found in 25% of cases (n = 313). The average left ventricular ejection fraction during acute TTC episodes was 40.2% (95% CI 38.3 to 42.1), increasing to 60.5% (95% CI 59.2 to 61.8) among the studies that followed up patients with TTC to recovery.
There were 96 deaths in the whole cohort. On meta-analysis, the in-hospital mortality was 4.5% (95% CI 3.1 to 6.2, I 2 = 60.8%). We performed comparisons between prospective and retrospective studies and between single- and multicenter studies to determine the substantial heterogeneity in mortality that might have arisen from these factors ( Table 2 ). There was no significant difference in mortality between studies of prospective and retrospective design, or between single- and multicenter studies.
| Grouping | Number of Studies | In-Hospital Death, % (95% CI) | I 2 |
|---|---|---|---|
| Total | 37 | 4.5 (3.1–6.2) | 60.8 |
| Retrospective studies | 18 | 4 (2.1–6.4) | 54.6 |
| Prospective studies | 12 | 4.8 (2.3–8.2) | 71.5 |
| Single-center studies | 28 | 4.9 (3.1–7.1) | 58.5 |
| Multicenter studies | 7 | 3.8 (1.4–7.1) | 74.8 |
Because of low numbers, a pooled analysis was performed for the cause of acute death ( Table 3 ), divided into cardiac and noncardiac origins. Among all deaths, 38% (n = 35) were directly related to cardiac complications and 62% (n = 58) to underlying co-morbid medical conditions. Ventricular arrhythmias, shock, and refractory heart failure contributed to most cardiac mortalities. In patients dying because of TTC-related cardiac complications, 40% (n = 14) died because of ventricular arrhythmias, 34% (n = 12) because of shock (n = 7) and acute heart failure (n = 5), and 26% (n = 9) had other cardiac complications (ventricular wall rupture, mural thrombus-related embolic complications, etc.).
| No. | First Author | Year of Publication | Deaths | Gender of Dead Patients | ||||
|---|---|---|---|---|---|---|---|---|
| Total | Cardiac | Underlying Medical Condition | Other | Male | Female | |||
| 1 | Spedicato | 2008 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2 | Elian | 2006 | 1 | 1 | 0 | 0 | 0 | 1 |
| 3 | Bonello | 2007 | 3 | 3 | 0 | 0 | 1 | 2 |
| 4 | Buja | 2012 | 2 | 1 | 1 | 0 | 1 | 1 |
| 5 | Hsu | 2010 | 0 | 0 | 0 | 0 | 0 | 0 |
| 6 | Sato | 2006 | 0 | 0 | 0 | 0 | 0 | 0 |
| 7 | Azzarelli | 2009 | 0 | 0 | 0 | 0 | 0 | 0 |
| 8 | Valbusa | 2008 | 2 | 0 | 0 | 2 | 0 | 0 |
| 9 | Kwon | 2012 | 18 | 0 | 14 | 4 | 8 | 10 |
| 10 | Primetshofer | 2010 | 0 | 0 | 0 | 0 | 0 | 0 |
| 11 | Eshtehardi | 2009 | 0 | 0 | 0 | 0 | 0 | 0 |
| 12 | Jabara | 2009 | 1 | 1 | 0 | 0 | 0 | 1 |
| 13 | Song | 2010 | 8 | 0 | 8 | 0 | 3 | 5 |
| 14 | Elesber | 2007 | 2 | 2 | 0 | 0 | NA | NA |
| 15 | Lee | 2010 | 9 | 6 | 3 | 0 | NA | NA |
| 16 | Vriz | 2013 | 2 | 1 | 1 | 0 | 0 | 2 |
| 17 | Sharkey | 2010 | 3 | 2 | 0 | 0 | 0 | 3 |
| 18 | Parodi | 2011 | 2 | 2 | 0 | 0 | 0 | 2 |
| 19 | Kurisu | 2010 | 7 | 0 | 6 | 1 | 2 | 5 |
| 20 | Joe | 2012 | 6 | 0 | 6 | 0 | 4 | 2 |
| 21 | Ionescu | 2010 | 0 | 0 | 0 | 0 | 0 | 0 |
| 22 | Kurowski | 2007 | 3 | 0 | 3 | 0 | NA | NA |
| 23 | Previtali | 2011 | 1 | 0 | 0 | 1 | NA | NA |
| 24 | Eitel | 2011 | 4 | 4 | 0 | 0 | 1 | 3 |
| 25 | Akashi | 2004 | 0 | 0 | 0 | 0 | 0 | 0 |
| 26 | Burgdorf | 2008 | 3 | 0 | 3 | 0 | NA | NA |
| 27 | Vidi | 2009 | 2 | 1 | 1 | 0 | NA | NA |
| 28 | Tsuchihashi | 2001 | 1 | 0 | 0 | 1 | NA | NA |
| 29 | Regnante | 2009 | 3 | 1 | 2 | 0 | NA | NA |
| 30 | Singh | 2010 | 1 | 1 | 0 | 0 | NA | NA |
| 31 | Yoshioka | 2008 | 4 | 0 | 4 | 0 | NA | NA |
| 32 | Mitsuma | 2010 | 0 | 0 | 0 | 0 | 0 | 0 |
| 33 | Herting | 2006 | 0 | 0 | 0 | 0 | 0 | 0 |
| 34 | Lee | 2009 | 3 | 0 | 3 | 0 | 2 | 1 |
| 35 | Fang | 2008 | 2 | 0 | 2 | 0 | 0 | 2 |
| 36 | Mitchell | 2007 | 0 | 0 | 0 | 0 | 0 | 0 |
| 37 | Athanasiadis | 2006 | 0 | 0 | 0 | 0 | 0 | 0 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


