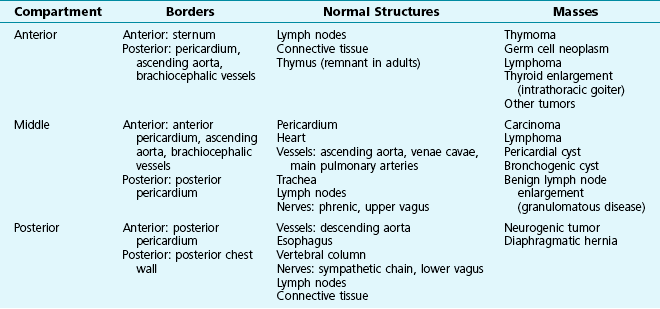
16 The mediastinum is bounded superiorly by bony structures of the thoracic inlet and inferiorly by the diaphragm. Laterally, the mediastinal pleura on each side serves as a membrane separating the medial aspect of the lung (with its visceral pleura) from the structures contained within the mediastinum. The mediastinum most frequently is divided into three anatomic compartments: anterior, middle, and posterior (Table 16-1). This division is particularly useful for characterizing mediastinal masses because specific etiologic factors often have a predilection for a particular compartment. Normal structures located within or coursing through each of the compartments may serve as the origin of a mediastinal mass. Consequently, knowledge of the structures contained in each of the three compartments is important for the clinician in evaluating a patient with a mediastinal mass. The borders of the three mediastinal compartments are visualized most easily on a lateral chest radiograph (Fig. 16-1). Several descriptions exist for the limits defining each compartment. According to the scheme used here, the anterior mediastinum extends from the sternum to the anterior border of the pericardium. Included within this region are the thymus, lymph nodes, and loose connective tissue. Because of the predilection for certain types of masses to occur in specific mediastinal compartments, it is easiest to separately consider masses occurring in each of the three anatomic regions. However, a fair amount of overlap occurs; that is, many types of mediastinal masses are not exclusively limited to the one compartment where they most frequently appear. A summary of the types of mediastinal masses, arranged by anatomic compartment, is given in Table 16-1.
Mediastinal Disease
Anatomic Features
Mediastinal Masses
Mediastinal Disease