Maximal Respiratory Pressures
In some clinical situations, evaluation of the strength of the respiratory muscles is very helpful. The strength of skeletal muscles, such as those of the arm, is easily tested by determining the force that they can develop, as by lifting weights. In contrast, the strength of the respiratory muscles can be determined by measuring the pressures developed against an occluded airway.
9A. Physiologic Principles
Some basic muscle physiology is reviewed here to aid in determining the best way of estimating the strength of respiratory muscles. Muscles, when maximally stimulated at different lengths, exhibit a characteristic length-tension behavior, as depicted in Figure 9-1. The greatest tension developed by the muscle occurs when it is at its optimal physiologic length. Less tension is developed at other lengths. To apply this concept to respiratory muscles, volume can be thought of as equivalent to length, and pressure as equivalent to tension. The expiratory muscles (chest wall and abdominal muscles) are at their optimal lengths near total lung capacity. Figure 9-2 shows, as expected, that the highest expiratory pressures are generated near total lung capacity. The subject blows as hard as possible against an occluded airway. Conversely, near residual volume, the inspiratory muscles (primarily the diaphragm) are at their optimal lengths. Near residual volume, they develop the most negative pressure when the subject is sucking against an occluded airway. Therefore, the maximal strength of the expiratory muscles is measured near total lung capacity and that of the inspiratory muscles is measured near residual volume.
9B. Measurement Techniques
The classic device used for these measurements is shown in Figure 9-3. It consists of a hollow stainless steel tube to which are attached negative- and positive-pressure gauges. The distal end of the tube is occluded, except for a 2-mm hole. Modern equipment has electronic pressure transducers connected to computer processors. Function is the same, but is less obvious on physical inspection.
Maximal expiratory pressure (PEmax) is measured as follows. The subject inhales maximally, holds the rubber tubing firmly against the mouth, and exhales as hard as possible. Several reproducible efforts are obtained, and the highest positive pressure maintained for 0.8 second is recorded. Firm rubber tubing is used rather than a standard snorkel-type mouthpiece because
at high pressures (150 cm H2O or more) air leaks around a conventional mouthpiece, the buccal muscles not being strong enough to maintain a tight seal. A nose clip is not usually required except for certain patients with severe muscle weakness.
at high pressures (150 cm H2O or more) air leaks around a conventional mouthpiece, the buccal muscles not being strong enough to maintain a tight seal. A nose clip is not usually required except for certain patients with severe muscle weakness.
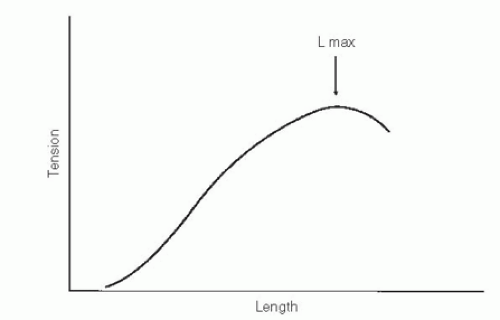 FIG. 9-1. Classic length-tension behavior of striated muscle. Lmax is the length at which maximal tension can be developed. |
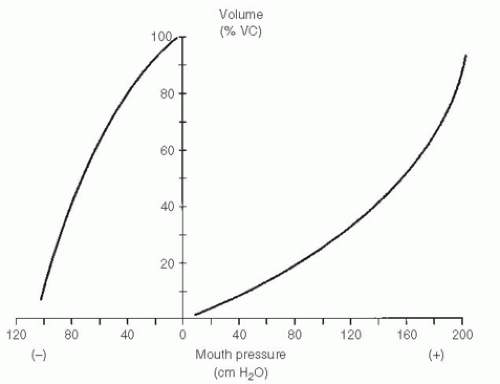 |
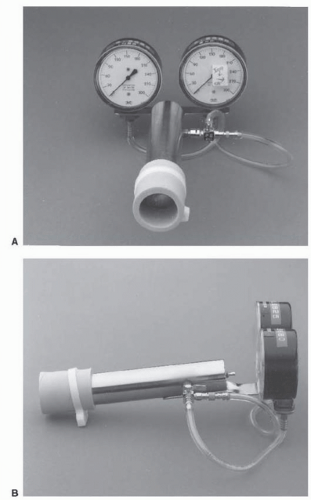 FIG. 9-3. Classical instrument used to measure maximal static expiratory and inspiratory pressures. The expiratory gauge measures 0 to +300 cm H2O, and the inspiratory gauge 0 to -300 cm H2O. Gauges are alternately connected to the cylinder by a three-way stopcock, as indicated by the arrows on the right-hand gauge (A). The side view (B) shows the small 2-mm hole at the distal end of the metal tube. A piece of firm rubber tubing is attached to the proximal end of the cylinder. |
TABLE 9-1. Normal Values for Maximal Respiratory Pressures, by Age
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|